Sasaki Tomohiko, Kunisaki Reiko, Kinoshita Hiroto, Kimura Hideaki, Kodera Teruaki, Nozawa Akinori, Hanzawa Akiho, Shibata Naomi, Yonezawa Hiromi, Miyajima Eiji, Morita Satoshi, Fujii Shoichi, Numata Kazushi, Tanaka Katsuaki, Tanaka Masanori, Maeda Shin
Inflammatory Bowel Disease Center, Yokohama City University Medical Center, Yokohama, Japan.
BMC Res Notes. 2014 Jun 14;7:363. doi: 10.1186/1756-0500-7-363.
Crohn's disease (CD) is routinely evaluated using clinical symptoms, laboratory variables, and the CD activity index (CDAI). However, clinical parameters are often nonspecific and do not precisely reflect the actual activity of CD small-intestinal lesions. The purposes of this prospective study were to compare color Doppler ultrasound (US) findings with histological findings from surgically resected specimens and confirm the hypothesis that color Doppler US can distinguish tissue inflammation and fibrosis.
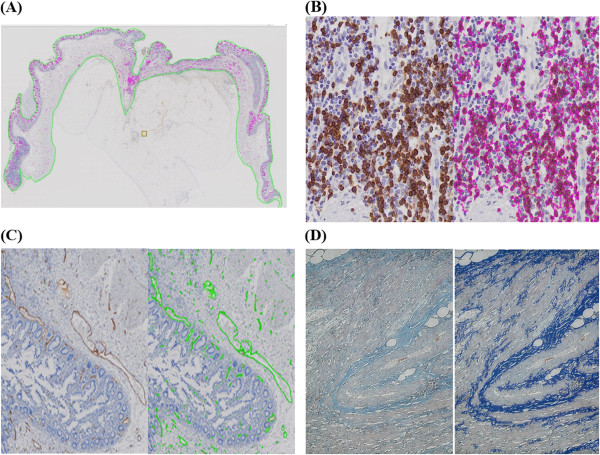
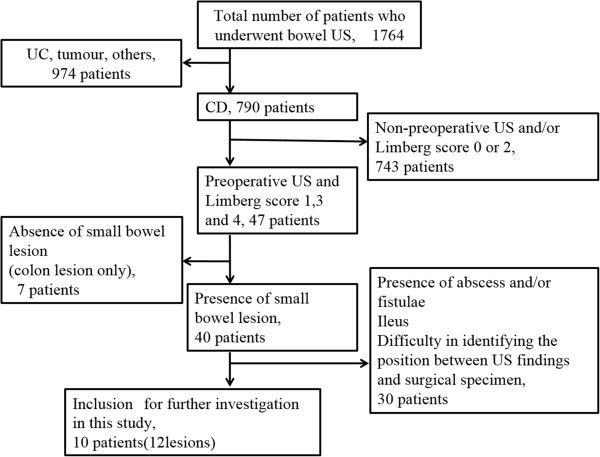
Among 1764 consecutive patients who underwent color Doppler US examinations, 10 patients with CD (12 small-intestinal CD lesions) who underwent US examinations before elective small-intestine resection were evaluated in the present study. Areas of thickened intestinal walls were evaluated in terms of blood flow using color Doppler US imaging. The blood flow was semiquantitatively classified as "hyper-flow" and "hypo-flow" according to the Limberg score. Resected lesions were macroscopically and histopathologically processed. Inflammatory cell infiltration, fibrosis and vascularity were evaluated by myeloperoxidase (granulocytes), CD163 (macrophages), CD79a (B cells), CD3 (T cells), Masson's trichrome (fibrosis), and factor VIII staining (vascular walls). All histopathological images were entered into virtual slide equipment and quantified using a quantitative microscopy integrated system (TissueMorph™).
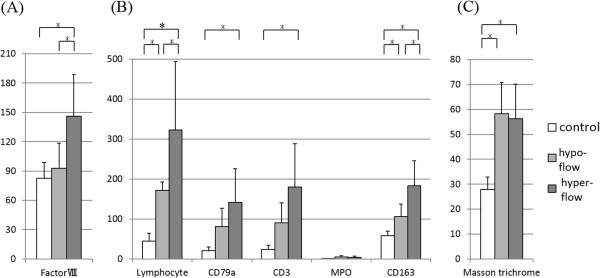
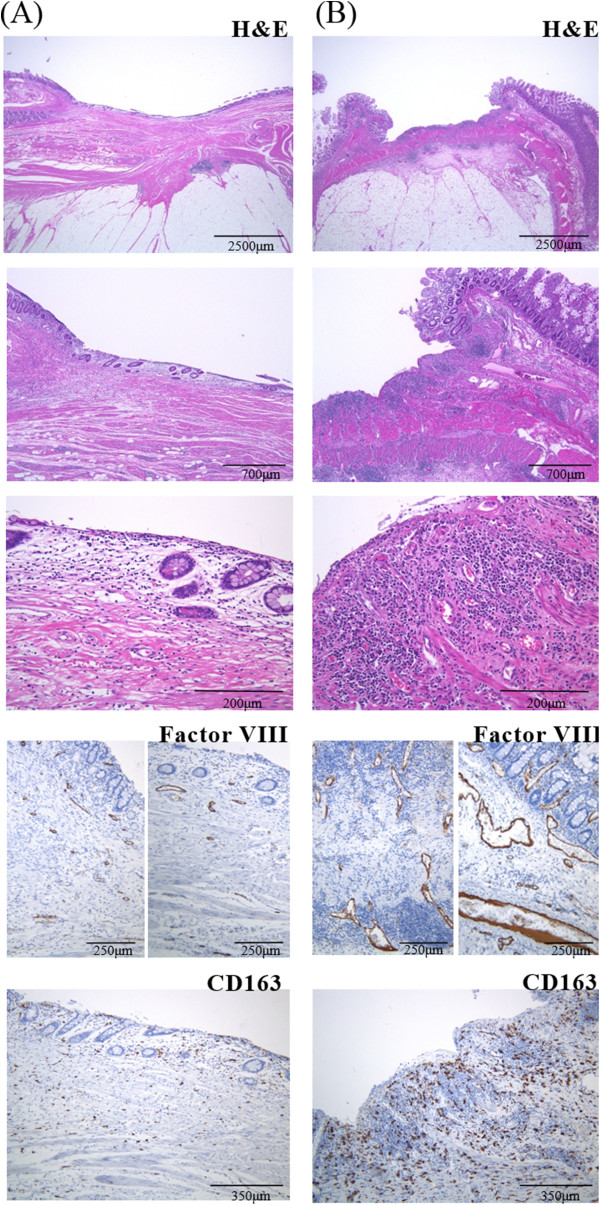
There were no significant differences in disease features or laboratory findings between "hypo-flow" lesions (n = 4) and "hyper-flow" lesions (n = 8). Histopathologically, "hyper-flow" lesions showed significantly greater bowel wall vascularity (factor VIII) (p = 0.047) and inflammatory cell infiltration, including CD163 macrophages (p = 0.008), CD3 T cells, and CD79a B cells (p = 0.043), than did "hypo-flow" lesions. There was no apparent association between the blood flow and CDAI.
In this study, active CD lesions were macroscopically visible in surgical specimens of patients with increased blood flow on preoperative color Doppler US imaging. Additionally, these CD lesions exhibited significantly greater vascularity and numbers of inflammatory leukocytes microscopically. Color Doppler US may predict tissue inflammation and fibrosis in small-intenstinal CD lesions.
克罗恩病(CD)通常采用临床症状、实验室指标及CD活动指数(CDAI)进行评估。然而,临床参数往往缺乏特异性,不能准确反映CD小肠病变的实际活动情况。本前瞻性研究旨在比较彩色多普勒超声(US)检查结果与手术切除标本的组织学检查结果,并验证彩色多普勒US能够区分组织炎症和纤维化这一假设。
在1764例连续接受彩色多普勒US检查的患者中,本研究评估了10例择期小肠切除术前接受US检查的CD患者(12处小肠CD病变)。采用彩色多普勒US成像评估肠壁增厚区域的血流情况。根据林贝格评分,血流情况被半定量分为“高血流”和“低血流”。对切除的病变进行大体和组织病理学处理。通过髓过氧化物酶(粒细胞)、CD163(巨噬细胞)、CD79a(B细胞)、CD3(T细胞)、马松三色染色法(纤维化)和因子VIII染色(血管壁)评估炎症细胞浸润、纤维化和血管形成情况。所有组织病理学图像均录入虚拟切片设备,并使用定量显微镜集成系统(TissueMorph™)进行定量分析。
“低血流”病变(n = 4)和“高血流”病变(n = 8)在疾病特征或实验室检查结果方面无显著差异。组织病理学检查显示,“高血流”病变的肠壁血管形成(因子VIII)(p = 0.047)及炎症细胞浸润,包括CD163巨噬细胞(p = 0.008)、CD3 T细胞和CD79a B细胞(p = 0.043)均显著多于“低血流”病变。血流情况与CDAI之间无明显关联。
在本研究中,术前彩色多普勒US成像显示血流增加的患者手术标本中,肉眼可见活动性CD病变。此外,这些CD病变在显微镜下显示出明显更多的血管形成和炎症白细胞数量。彩色多普勒US可能预测小肠CD病变中的组织炎症和纤维化。