Institute of Clinical Medicine, The Arctic University of Norway, Tromso, Norway.
BMC Urol. 2014 Jun 14;14:49. doi: 10.1186/1471-2490-14-49.
Prostate cancer is the most common male malignancy and a mayor cause of mortality in the western world. The impact of clinicopathological variables on disease related outcomes have mainly been reported from a few large US series, most of them not reporting on perineural infiltration. We therefore wanted to investigate relevant cancer outcomes in patients undergoing radical prostatectomy in two Norwegian health regions with an emphasis on the impact of perineural infiltration (PNI) and prostate specific antigen- doubling time (PSA-DT).
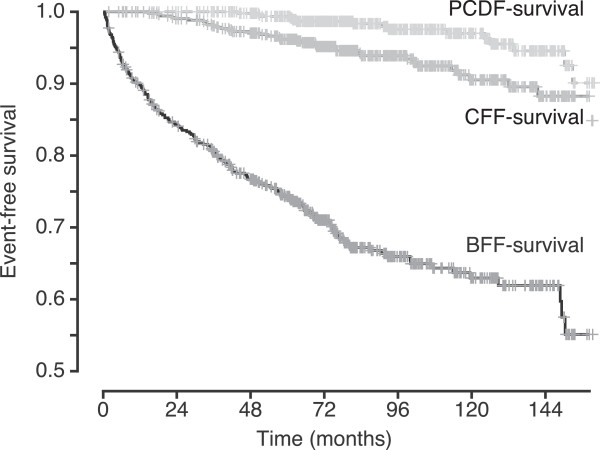
We conducted a retrospective analysis of 535 prostatectomy patients at three hospitals between 1995 and 2005 estimating biochemical failure- (BFFS), clinical failure- (CFFS) and prostate cancer death-free survival (PCDFS) with the Kaplan-Meier method. We investigated clinicopathological factors influencing risk of events using cox proportional hazard regression.
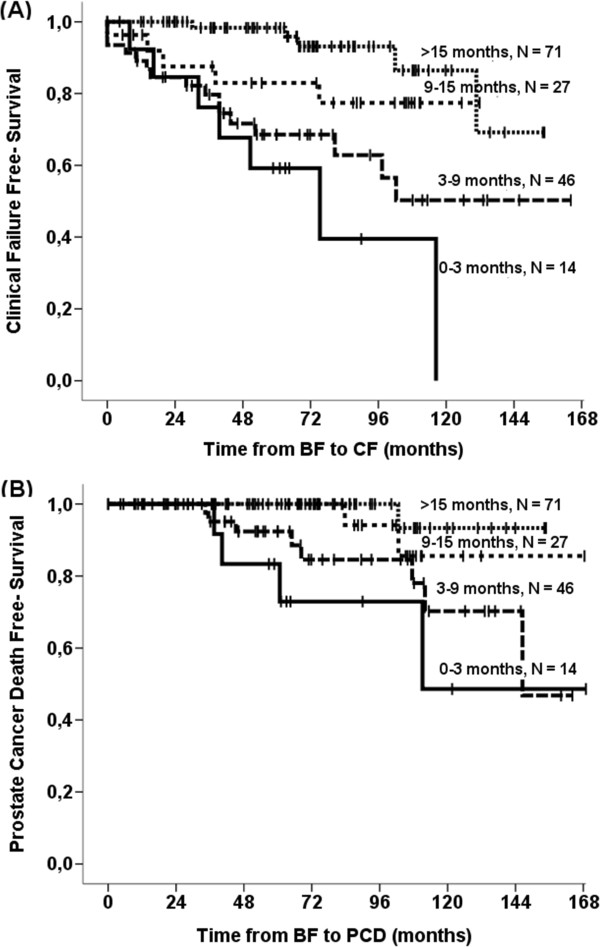
After a median follow-up of 89 months, 170 patients (32%) experienced biochemical failure (BF), 36 (7%) experienced clinical failure and 15 (3%) had died of prostate cancer. pT-Stage (p = 0.001), preoperative PSA (p = 0.047), Gleason Score (p = 0.032), non-apical positive surgical margins (PSM) (p = 0.003) and apical PSM (p = 0.031) were all independently associated to BFFS. Gleason score (p = 0.019), PNI (p = 0.012) and non-apical PSM (p = 0.002) were all independently associated to CFFS while only PNI (P = 0.047) and subgroups of Gleason score were independently associated to PCDFS. After BF, patients with a shorter PSA-DT had independent and significant worse event-free survivals than patients with PSA-DT > 15 months (PSA-DT = 3-9 months, CFFS HR = 6.44, p < 0.001, PCDFS HR = 13.7, p = 0.020; PSA-DT < 3 months, CFFS HR = 11.2, p < 0.001, PCDFS HR = 27.5, p = 0.006).
After prostatectomy, CFFS and PCDFS are variable, but both are strongly associated to Gleason score and PNI. In patients with BF, PSA-DT was most strongly associated to CF and PCD. Our study adds weight to the importance of PSA-DT and re-launches PNI as a strong prognosticator for clinically relevant endpoints.
前列腺癌是男性最常见的恶性肿瘤,也是西方世界男性死亡的主要原因之一。临床病理变量对疾病相关结局的影响主要来自于少数美国大型系列研究,其中大多数研究并未报告神经周围浸润情况。因此,我们希望研究在两个挪威卫生区接受根治性前列腺切除术的患者的相关癌症结局,并重点研究神经周围浸润(PNI)和前列腺特异性抗原倍增时间(PSA-DT)的影响。
我们对 1995 年至 2005 年间在三家医院接受前列腺切除术的 535 名患者进行了回顾性分析,采用 Kaplan-Meier 法估计生化失败(BFFS)、临床失败(CFFS)和前列腺癌无死亡生存(PCDFS)。我们使用 Cox 比例风险回归来研究影响事件风险的临床病理因素。
中位随访 89 个月后,170 名患者(32%)出现生化失败(BF),36 名(7%)出现临床失败,15 名(3%)死于前列腺癌。pT 期(p=0.001)、术前 PSA(p=0.047)、Gleason 评分(p=0.032)、非顶点切缘阳性(p=0.003)和顶点切缘阳性(p=0.031)均与 BFFS 独立相关。Gleason 评分(p=0.019)、PNI(p=0.012)和非顶点切缘阳性(p=0.002)均与 CFFS 独立相关,而只有 PNI(p=0.047)和 Gleason 评分亚组与 PCDFS 独立相关。在 BF 后,PSA-DT 较短的患者无事件生存明显差于 PSA-DT>15 个月的患者(PSA-DT=3-9 个月,CFFS HR=6.44,p<0.001,PCDFS HR=13.7,p=0.020;PSA-DT<3 个月,CFFS HR=11.2,p<0.001,PCDFS HR=27.5,p=0.006)。
前列腺切除术后,CFFS 和 PCDFS 是可变的,但均与 Gleason 评分和 PNI 密切相关。在 BF 患者中,PSA-DT 与 CF 和 PCD 最密切相关。我们的研究进一步证实了 PSA-DT 的重要性,并重新将 PNI 作为临床相关终点的一个强有力的预后因素。