Hayashi Katsuhiro, Iwata Shintaro, Ogose Akira, Kawai Akira, Ueda Takafumi, Otsuka Takanobu, Tsuchiya Hiroyuki
Department of Orthopaedic Surgery, Graduate School of Medical Science, Kanazawa University, Kanazawa, Japan; Department of Orthopaedic Surgery, Nagoya City University Medical School, Nagoya, Japan.
Division of Orthopedic Surgery, Chiba Cancer Center, Chiba, Japan.
PLoS One. 2014 Jun 17;9(6):e100119. doi: 10.1371/journal.pone.0100119. eCollection 2014.
Scapulectomy requires not only joint resection but also wide resection of the shoulder girdle muscles. Even the significance of reconstruction has not yet been determined because of the difficulties in comparing the different conditions. The purpose of this study was to investigate factors that influence functional outcomes after scapulectomy in a multicenter study.
This retrospective study comprised 48 patients who underwent total or subtotal scapulectomy and were followed for at least one year after surgery. Patients were registered at the Japanese Musculoskeletal Oncology Group affiliated hospitals. Soft tissue reconstruction for joint stabilization was performed when there was enough remaining tissue for reconstruction of the rotator cuff and tendons. In 23 cases, humeral suspension was performed. The average follow-up period was 61.9 months. Multivariate analysis was performed using the patient's background to determine which factors influence the Enneking functional score or active range of motion.
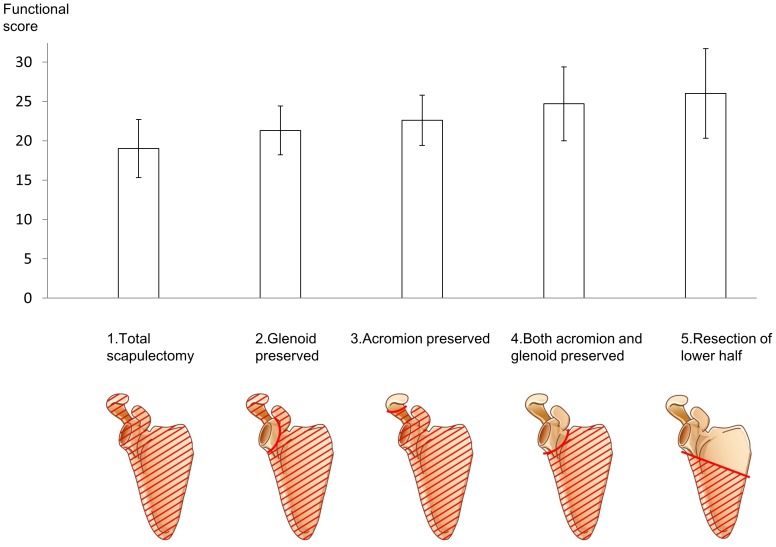
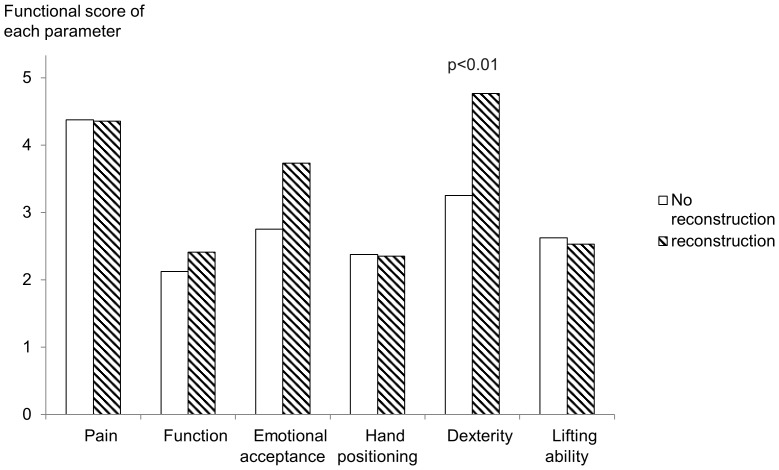
The average functional score was 21.1 out of 30. Active shoulder range of motion was 42.7 degree in flexion, 39.7 degree in abduction, 49.6 degree of internal rotation and 16.8 degree of external rotation. The amount of remaining bone influenced functional outcome, which means that preserving the glenoid or the acromion lead to better function compared to total scapulectomy (p<0.01). Factors that influenced each functional measure include the amount of remaining bone, soft tissue reconstruction, the length of the resected humerus and nerve resection (p<0.05).
Although shoulder function was almost eliminated following total or subtotal scapulectomy, minimal resection of bone, and soft tissue reconstruction should lead to better function.
肩胛骨切除术不仅需要进行关节切除,还需要广泛切除肩胛带肌肉。由于难以比较不同情况,重建的意义尚未确定。本研究的目的是在一项多中心研究中调查影响肩胛骨切除术后功能结果的因素。
这项回顾性研究纳入了48例行全肩胛骨切除或次全肩胛骨切除且术后至少随访1年的患者。患者在日本肌肉骨骼肿瘤学组附属医院登记。当有足够的剩余组织用于重建肩袖和肌腱以稳定关节时,进行软组织重建。23例患者进行了肱骨悬吊术。平均随访期为61.9个月。使用患者的背景资料进行多变量分析,以确定哪些因素会影响Enneking功能评分或活动范围。
平均功能评分为30分中的21.1分。肩关节活动范围为前屈42.7度、外展39.7度、内旋49.6度和外旋16.8度。剩余骨量影响功能结果,这意味着与全肩胛骨切除术相比,保留肩胛盂或肩峰可导致更好的功能(p<0.01)。影响各项功能指标的因素包括剩余骨量、软组织重建、切除肱骨的长度和神经切除(p<0.05)。
尽管全肩胛骨切除或次全肩胛骨切除后肩部功能几乎丧失,但最小限度的骨切除和软组织重建应能带来更好的功能。