Kaltsonoudis Evripidis, Zikou Anastasia K, Voulgari Paraskevi V, Konitsiotis Spyridon, Argyropoulou Maria I, Drosos Alexandros A
Arthritis Res Ther. 2014 Jun 17;16(3):R125. doi: 10.1186/ar4582.
The aim was to investigate the frequency of neurological adverse events in patients with rheumatoid arthritis (RA) and spondylarthropathies (SpA) treated with tumor necrosis factor (TNF) α antagonists.
Seventy-seven patients eligible for anti-TNFα therapy were evaluated. There were 36 patients with RA, 41 with SpA [24 psoriatic arthritis (PsA) and 17 with ankylosing spondylitis (AS)]. All patients had a complete physical and neurological examination. Brain and cervical spine magnetic resonance imaging (MRI) and neurophysiological tests were performed in all patients before the initiation of anti-TNFα therapy and after a mean of 18 months or when clinical symptoms and signs indicated a neurological disease. Exclusion criteria included hypertension, diabetes mellitus, dyslipidemia, heart arrhythmias, atherothrombotic events, vitamin B12 and iron deficiency, head and neck trauma and neurological surgeries.
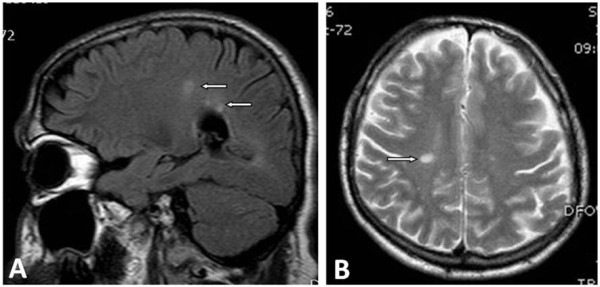
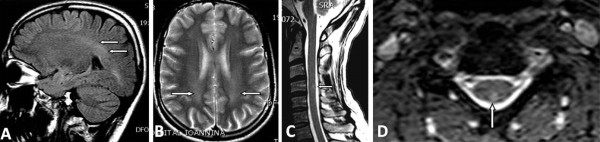
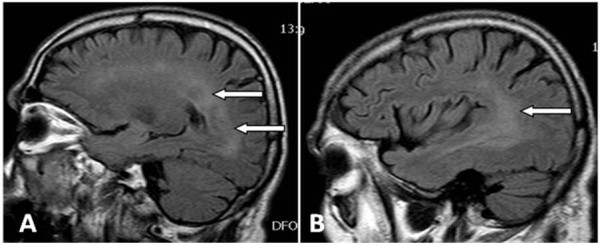
Two patients did not receive anti-TNFα therapy because brain MRIs at baseline revealed lesions compatible with demyelinating diseases. Thus, 75 patients received anti-TNFα (38 infliximab, 19 adalimumab and 18 etanercept). Three patients developed neurological adverse events. A 35-year-old man with PsA after 8 months of infliximab therapy presented with paresis of the left facial nerve and brain MRI showed demyelinating lesions. Infliximab was discontinued and he was treated with pulses of corticosteroids recovering completely after two months. The second patient was a 45-year-old woman with RA who after 6 months of adalimumab therapy presented with optic neuritis. The third patient was a 50-year-old woman with AS, whom after 25 months of infliximab therapy, presented with tingling and numbness of the lower extremities and neurophysiological tests revealed peripheral neuropathy. In both patients anti-TNF were discontinued and they improved without treatment after 2 months. The rest of our patients showed no symptoms and MRIs showed no abnormalities. The estimated rate of neurological adverse events in patients treated with anti-TNF therapy is 4% (3/75).
Neurological adverse events after anti-TNFα therapy were observed in our patient. Brain MRI and neurophysiological tests are essential tools to discriminate neurological diseases.
目的是调查接受肿瘤坏死因子(TNF)α拮抗剂治疗的类风湿关节炎(RA)和脊柱关节炎(SpA)患者中神经不良事件的发生频率。
对77例符合抗TNFα治疗条件的患者进行了评估。其中36例为RA患者,41例为SpA患者[24例银屑病关节炎(PsA)和17例强直性脊柱炎(AS)]。所有患者均进行了全面的体格和神经系统检查。在开始抗TNFα治疗前以及平均18个月后或出现临床症状和体征提示神经系统疾病时,对所有患者进行了脑和颈椎磁共振成像(MRI)以及神经生理学检查。排除标准包括高血压、糖尿病、血脂异常、心律失常、动脉粥样硬化血栓形成事件、维生素B12和铁缺乏、头颈部创伤以及神经外科手术。
2例患者因基线脑MRI显示与脱髓鞘疾病相符的病变而未接受抗TNFα治疗。因此,75例患者接受了抗TNFα治疗(38例英夫利昔单抗、19例阿达木单抗和18例依那西普)。3例患者发生了神经不良事件。1例35岁的PsA男性在接受英夫利昔单抗治疗8个月后出现左侧面神经麻痹,脑MRI显示脱髓鞘病变。停用英夫利昔单抗,给予糖皮质激素冲击治疗,2个月后完全康复。第二例患者是一名45岁的RA女性,在接受阿达木单抗治疗6个月后出现视神经炎。第三例患者是一名50岁的AS女性,在接受英夫利昔单抗治疗25个月后出现下肢刺痛和麻木,神经生理学检查显示为周围神经病变。这两名患者均停用了抗TNF药物,2个月后未经治疗病情好转。其余患者均未出现症状,MRI也未显示异常。接受抗TNF治疗的患者中神经不良事件的估计发生率为4%(3/75)。
我们的患者中观察到了抗TNFα治疗后的神经不良事件。脑MRI和神经生理学检查是鉴别神经系统疾病的重要工具。