Saira Dars, MS Obstetrics & Gynaecology, Department of Obstetrics & Gynaecology, Liaquat University Hospital, Hyderabad, Sindh, Pakistan.
Safia Malik, Postgraduate Scholar Obstetrics & Gynaecology, Department of Obstetrics & Gynaecology, Liaquat University Hospital, Hyderabad, Sindh, Pakistan.
Pak J Med Sci. 2014 May;30(3):626-9. doi: 10.12669/pjms.303.4853.
To assess the maternal morbidity and perinatal outcome in pre-term pre mature rupture of membranes between 24 to 37 weeks gestation.
This observational study was carried out in Gynaecology & Obstetrics Unit - I, at University Hospital Hyderabad, from October 2010 to October 2011. It included one hundred patients admitted through the outpatient department, as well as from casualty department of University Hospital Hyderabad. Detailed Clinical examination of the patient was done. Systemic review was also done to see any co-morbidity. All patients had laboratory investigations. Inclusion criteria were all patients gestational age between 24 to 37 weeks with preterm premature rupture of membrane (PPROM) confirmed by ultrasound and clinical examination regardless of their age. Exclusion criteria were patients with congenital anomalies, multiple pregnancy, pre-eclampsia & eclampsia, diabetes mellitus, polyhydramnios1 intrauterine growth restriction and placenta abruption. Data was collected using a proforma. Detailed workup including history, general physical examination, abdomen and pelvic examination and relevant specific investigations were noted.
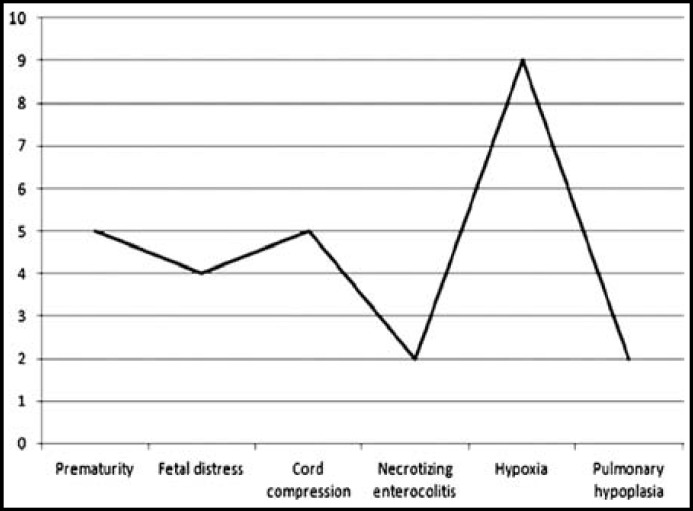
Out of 100 patients included in this study Primigravida were 17% and multigravida 83%. There was wide variation of age ranging from a minimum of 20to >40 years. The mean age was 30+ 3.1 years. Mostly patients belonged to the poor class in 72% cases followed by middle class in 21% and upper class 7%. Analysis shows that out of 100 mothers 26% had PROM of <24 hrs duration and 74% had >24 hrs of duration. Maternal outcome in 16 cases of Preterm Premature Rupture of Membrane findings revealed septicemia in 12% cases and Chorioamnionitis in 12% cases. Fetal outcome in 27 cases of preterm premature rupture of membrane revealed prematurity in 5% cases, fetal distress in 4% cases, cord compression in 5% cases, necrotizing enterocolitis in 2% cases, hypoxia in 9% cases and pulmonary hypoplasia in 2% cases.
Low socioeconomic status is associated with increased neonatal morbidity due to fetal distress, cord compression, necrotizing enterocolitis, hypoxia and pulmonary hypoplasia at the time of delivery. An appropriate and accurate diagnosis of PROM is critical to optimize pregnancy outcome. It is suggested that the timely diagnosis and management of preterm PROM will allow obstetric care providers to optimize perinatal outcome and minimize neonatal morbidity.
评估 24 至 37 周妊娠早产胎膜早破的产妇发病率和围产儿结局。
本观察性研究于 2010 年 10 月至 2011 年 10 月在海得拉巴大学医院妇产科 I 病房进行。研究纳入了通过门诊部和海得拉巴大学医院急诊室入院的 100 名患者。对患者进行了详细的临床检查,并进行了系统回顾以了解是否存在合并症。所有患者均进行了实验室检查。纳入标准为所有 24 至 37 周妊娠且经超声和临床检查证实为早产胎膜早破(PPROM)的患者,无论其年龄大小。排除标准为患有先天性畸形、多胎妊娠、子痫前期/子痫、糖尿病、羊水过多、宫内生长受限和胎盘早剥的患者。使用表格收集数据。详细的检查包括病史、一般体格检查、腹部和骨盆检查以及相关的特定检查。
本研究共纳入 100 名患者,初产妇占 17%,经产妇占 83%。年龄从最小的 20 岁到最大的>40 岁不等,差异较大。平均年龄为 30+3.1 岁。大多数患者属于贫困阶层,占 72%,其次是中产阶级,占 21%,上层阶级占 7%。分析显示,在 100 名母亲中,有 26%的胎膜早破持续时间<24 小时,74%的胎膜早破持续时间>24 小时。16 例早产胎膜早破的产妇中,有 12%发生败血症,12%发生绒毛膜羊膜炎。27 例早产胎膜早破的胎儿结局显示,5%的新生儿早产,4%的新生儿出现胎儿窘迫,5%的新生儿出现脐带受压,2%的新生儿出现坏死性小肠结肠炎,9%的新生儿出现缺氧,2%的新生儿出现肺发育不良。
由于分娩时胎儿窘迫、脐带受压、坏死性小肠结肠炎、缺氧和肺发育不良,社会经济地位较低与新生儿发病率增加有关。对 PROM 的准确和适当诊断对于优化妊娠结局至关重要。建议及时诊断和处理早产胎膜早破,以便产科护理人员优化围产儿结局,最大限度地减少新生儿发病率。