Department of Respiratory Medicine, Japanese Red Cross Medical Centre, 4-1-22 Hiroo, Shibuyaku, Tokyo 150-8953, Japan.
BMC Pulm Med. 2014 Jun 28;14:104. doi: 10.1186/1471-2466-14-104.
Clinical evaluation to differentiate the characteristic features of pulmonary fibrosis and emphysema is often difficult in patients with combined pulmonary fibrosis and emphysema (CPFE), but diagnosis of pulmonary fibrosis is important for evaluating treatment options and the risk of acute exacerbation of interstitial pneumonia of such patients. As far as we know, it is the first report describing a correlation among clinical, radiological, and whole-lung pathological features in an autopsy cases of CPFE patients.
Experts retrospectively reviewed the clinical charts and examined chest computed tomography (CT) images and pathological findings of an autopsy series of 22 CPFE patients, and compared these with findings from 8 idiopathic pulmonary fibrosis (IPF) patients and 17 emphysema-alone patients.
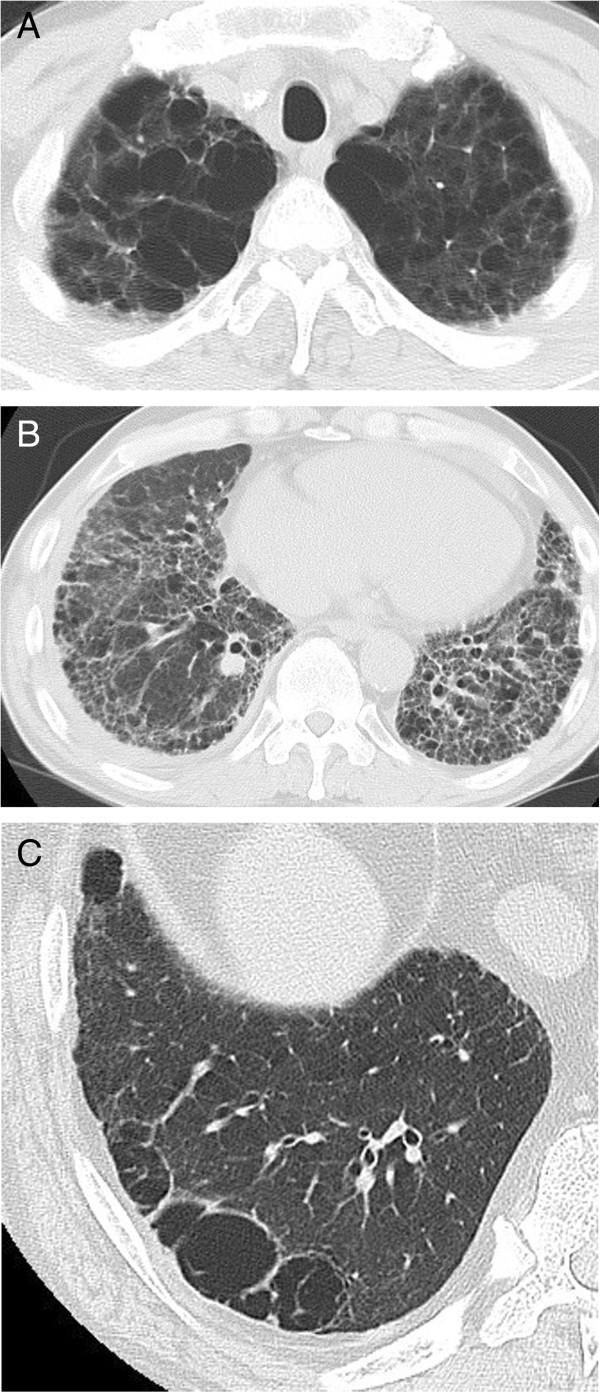
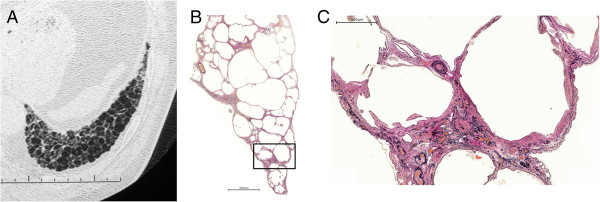
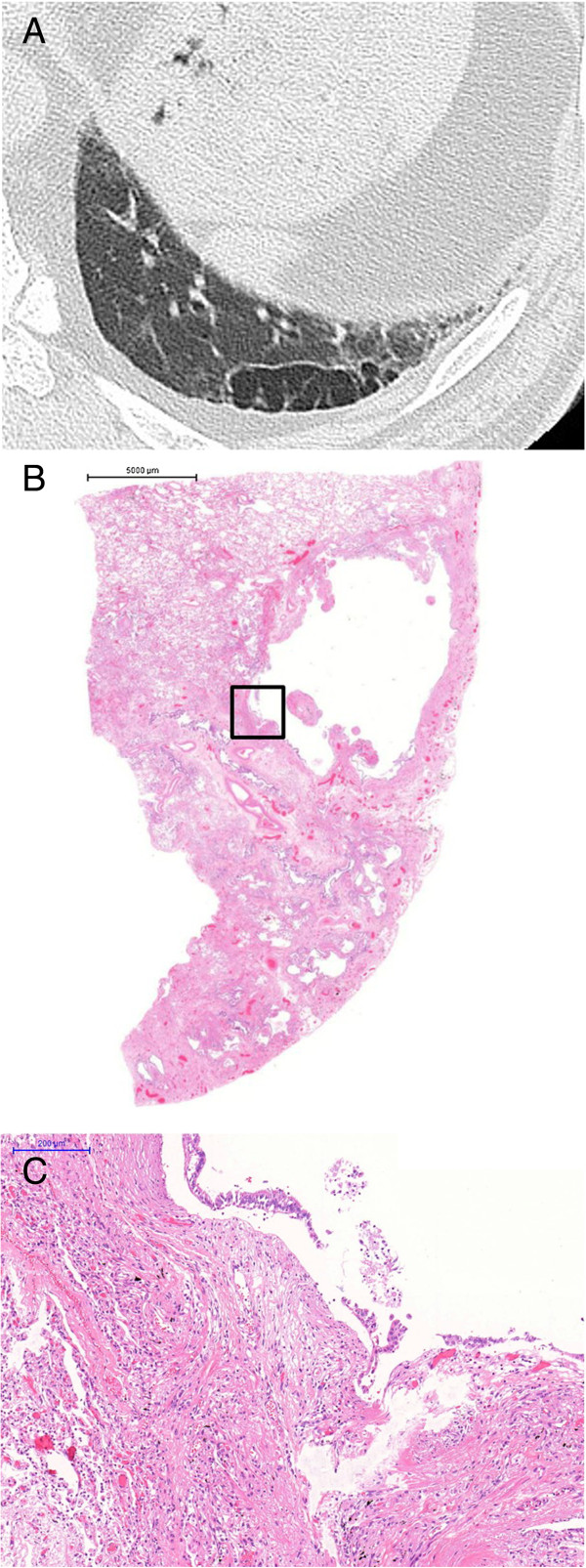
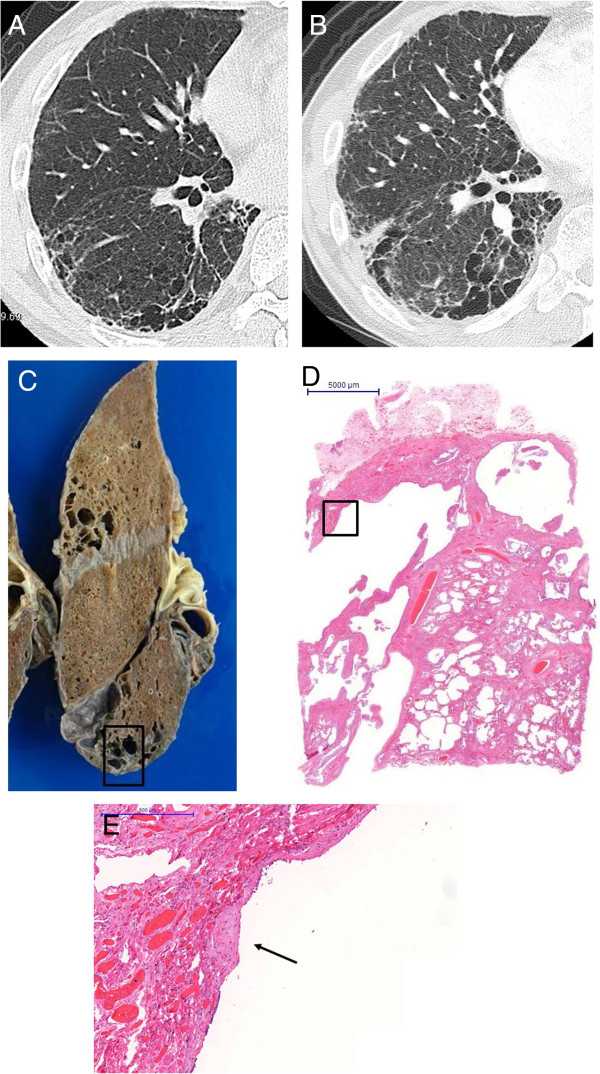
All patients had a history of heavy smoking. Forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC%) was significantly lower in the emphysema-alone group than the CPFE and IPF-alone groups. The percent predicted diffusing capacity of the lung for carbon monoxide (DLCO%) was significantly lower in the CPFE group than the IPF- and emphysema-alone groups. Usual interstitial pneumonia (UIP) pattern was observed radiologically in 15 (68.2%) CPFE and 8 (100%) IPF-alone patients and was pathologically observed in all patients from both groups. Pathologically thick-cystic lesions involving one or more acini with dense wall fibrosis and occasional fibroblastic foci surrounded by honeycombing and normal alveoli were confirmed by post-mortem observation as thick-walled cystic lesions (TWCLs). Emphysematous destruction and enlargement of membranous and respiratory bronchioles with fibrosis were observed in the TWCLs. The cystic lesions were always larger than the cysts of honeycombing. The prevalence of both radiological and pathological TWCLs was 72.7% among CPFE patients, but no such lesions were observed in patients with IPF or emphysema alone (p=0.001). The extent of emphysema in CPFE patients with TWCLs was greater than that in patients without such lesions. Honeycombing with emphysema was also observed in 11 CPFE patients.
TWCLs were only observed in the CPFE patients. They were classified as lesions with coexistent fibrosing interstitial pneumonia and emphysema, and should be considered an important pathological and radiological feature of CPFE.
在合并肺纤维化和肺气肿(CPFE)患者中,临床评估常常难以区分肺纤维化和肺气肿的特征,但诊断肺纤维化对于评估此类患者的治疗选择和间质性肺炎急性加重的风险很重要。据我们所知,这是首例描述 CPFE 患者尸检病例中临床、影像学和全肺病理学特征之间相关性的报告。
专家回顾性地审查了 22 例 CPFE 患者的临床病历,并检查了胸部计算机断层扫描(CT)图像和尸检结果,将这些结果与 8 例特发性肺纤维化(IPF)患者和 17 例单纯肺气肿患者的结果进行了比较。
所有患者均有大量吸烟史。单纯肺气肿组用力肺活量(FEV1/FVC%)明显低于 CPFE 和 IPF 组。CPFE 组预测的一氧化碳弥散量(DLCO%)明显低于 IPF 和单纯肺气肿组。15 例(68.2%)CPFE 和 8 例(100%)IPF 患者的影像学表现为寻常型间质性肺炎(UIP)模式,两组所有患者的病理检查均观察到 UIP 模式。通过尸检观察证实,病理上厚壁囊性病变累及一个或多个腺泡,伴有致密壁纤维化和偶尔纤维化灶周围的蜂窝状改变和正常肺泡,为厚壁囊性病变(TWCL)。在 TWCL 中观察到膜性和呼吸细支气管的气肿性破坏和纤维化导致的扩张。囊性病变总是大于蜂窝状的囊肿。CPFE 患者中 TWCL 的影像学和病理学患病率均为 72.7%,但在 IPF 或单纯肺气肿患者中未观察到此类病变(p=0.001)。TWCL 阳性 CPFE 患者的肺气肿程度大于无此类病变的患者。在 11 例 CPFE 患者中也观察到伴气肿的蜂窝状改变。
TWCL 仅在 CPFE 患者中观察到。它们被归类为同时存在纤维化性间质性肺炎和肺气肿的病变,应被视为 CPFE 的一个重要的病理和影像学特征。