Blum Claudine A, Nigro Nicole, Winzeler Bettina, Suter-Widmer Isabelle, Schuetz Philipp, Briel Matthias, Bingisser Roland, Zimmerli Werner, Ullmer Elke, Elsaesser Hanno, Tarr Philip, Wirz Sebastian, Thomann Robert, Hofmann Eveline, Rodondi Nicolas, Duplain Hervé, Burki Dieter, Mueller Beat, Christ-Crain Mirjam
Endocrinology, Diabetology and Metabolism, Department of Internal Medicine, University Hospital Basel, Petersgraben 4, 4031 Basel, Switzerland.
Trials. 2014 Jun 28;15:257. doi: 10.1186/1745-6215-15-257.
Community-acquired pneumonia (CAP) is the third-leading infectious cause of death worldwide. The standard treatment of CAP has not changed for the past fifty years and its mortality and morbidity remain high despite adequate antimicrobial treatment. Systemic corticosteroids have anti-inflammatory effects and are therefore discussed as adjunct treatment for CAP. Available studies show controversial results, and the question about benefits and harms of adjunct corticosteroid therapy has not been conclusively resolved, particularly in the non-critical care setting.
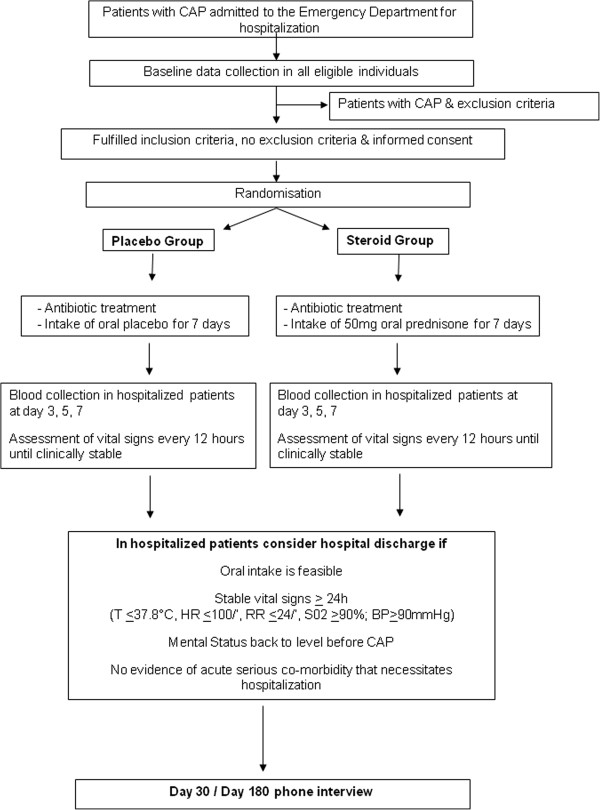
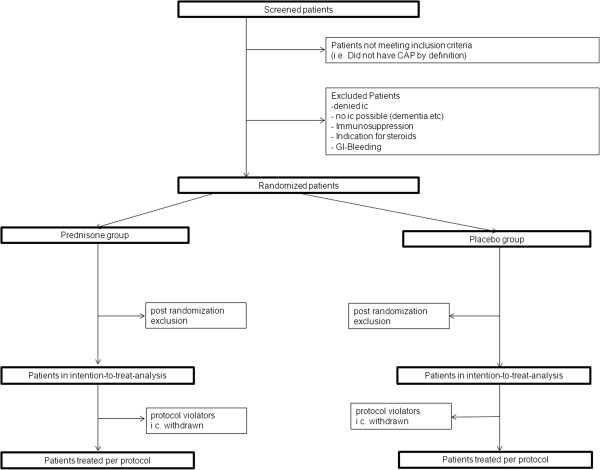
METHODS/DESIGN: This randomized multicenter study compares a treatment with 7 days of prednisone 50 mg with placebo in adult patients hospitalized with CAP independent of severity. Patients are screened and enrolled within the first 36 hours of presentation after written informed consent is obtained. The primary endpoint will be time to clinical stability, which is assessed every 12 hours during hospitalization. Secondary endpoints will be, among others, all-cause mortality within 30 and 180 days, ICU stay, duration of antibiotic treatment, disease activity scores, side effects and complications, value of adrenal function testing and prognostic hormonal and inflammatory biomarkers to predict outcome and treatment response to corticosteroids. Eight hundred included patients will provide an 85% power for the intention-to-treat analysis of the primary endpoint.
This largest to date double-blind placebo-controlled multicenter trial investigates the effect of adjunct glucocorticoids in 800 patients with CAP requiring hospitalization. It aims to give conclusive answers about benefits and risks of corticosteroid treatment in CAP. The inclusion of less severe CAP patients will be expected to lead to a relatively low mortality rate and survival benefit might not be shown. However, our study has adequate power for the clinically relevant endpoint of clinical stability. Due to discontinuing glucocorticoids without tapering after seven days, we limit duration of glucocorticoid exposition, which may reduce possible side effects.
7 September 2009 on ClinicalTrials.gov: NCT00973154.
社区获得性肺炎(CAP)是全球第三大感染性死亡原因。在过去的五十年里,CAP的标准治疗方法没有改变,尽管进行了充分的抗菌治疗,但其死亡率和发病率仍然很高。全身用皮质类固醇具有抗炎作用,因此被作为CAP的辅助治疗方法进行讨论。现有研究结果存在争议,关于辅助皮质类固醇治疗的利弊问题尚未得到最终解决,尤其是在非重症监护环境中。
方法/设计:这项随机多中心研究比较了50毫克泼尼松治疗7天与安慰剂治疗对因CAP住院的成年患者(无论病情严重程度)的效果。在获得书面知情同意后,患者在就诊后的前36小时内接受筛查并入组。主要终点将是临床稳定时间,住院期间每12小时评估一次。次要终点包括30天和180天内的全因死亡率、入住重症监护病房(ICU)的时间、抗生素治疗时间、疾病活动评分、副作用和并发症、肾上腺功能测试值以及预测结果和对皮质类固醇治疗反应的预后激素和炎症生物标志物等。纳入的800名患者将为主要终点的意向性分析提供85%的检验效能。
这项迄今为止规模最大的双盲安慰剂对照多中心试验研究了辅助糖皮质激素对800例需要住院治疗的CAP患者的影响。其目的是就皮质类固醇治疗CAP的利弊给出确凿答案。纳入病情较轻的CAP患者预计会导致相对较低的死亡率,可能不会显示出生存获益。然而,我们的研究对于临床稳定这一临床相关终点具有足够的检验效能。由于在7天后不逐渐减量就停用糖皮质激素,我们限制了糖皮质激素的暴露时间,这可能会减少可能的副作用。
2009年9月7日在ClinicalTrials.gov注册:NCT00973154。