Olfert I Mark, Malek Moh H, Eagan Tomas M L, Wagner Harrieth, Wagner Peter D
Center for Cardiovascular and Respiratory Sciences, Division of Exercise Physiology, One Medical Center Dr, West Virginia University School of Medicine, Morgantown, WV 26506-9105, USA.
BMC Pulm Med. 2014 Jun 30;14:106. doi: 10.1186/1471-2466-14-106.
There is still limited information on systemic inflammation in alpha-1-antitrypsin-deficient (AATD) COPD patients and what effect alpha-1-antitrypsin augmentation therapy and/or exercise might have on circulating inflammatory cytokines. We hypothesized that AATD COPD patients on augmentation therapy (AATD + AUG) would have lower circulating and skeletal muscle inflammatory cytokines compared to AATD COPD patients not receiving augmentation therapy (AATD-AUG) and/or the typical non-AATD (COPD) patient. We also hypothesized that cytokine response to exercise would be lower in AATD + AUG compared to AATD-AUG or COPD subjects.
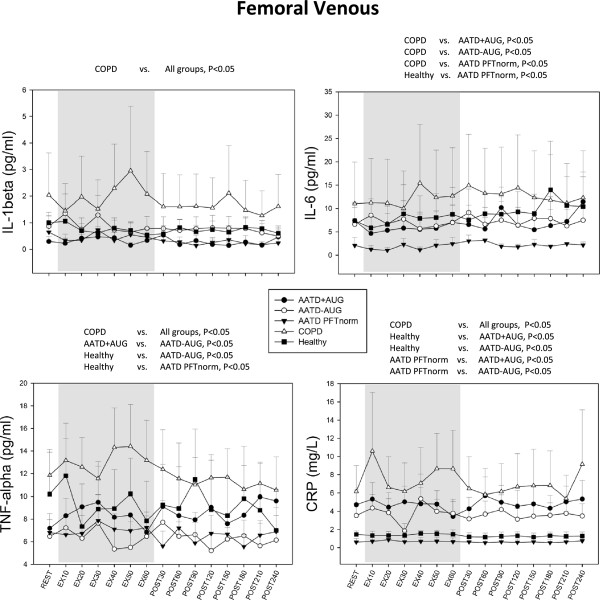
Arterial and femoral venous concentration and skeletal muscle expression of TNFα, IL-6, IL-1β and CRP were measured at rest, during and up to 4-hours after 50% maximal 1-hour knee extensor exercise in all COPD patient groups, including 2 additional groups (i.e. AATD with normal lung function, and healthy age-/activity-matched controls).
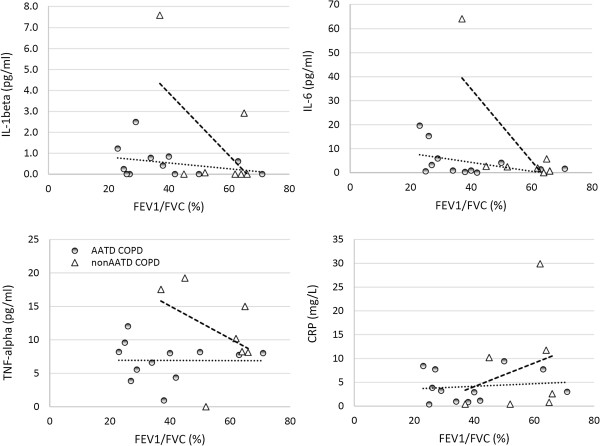
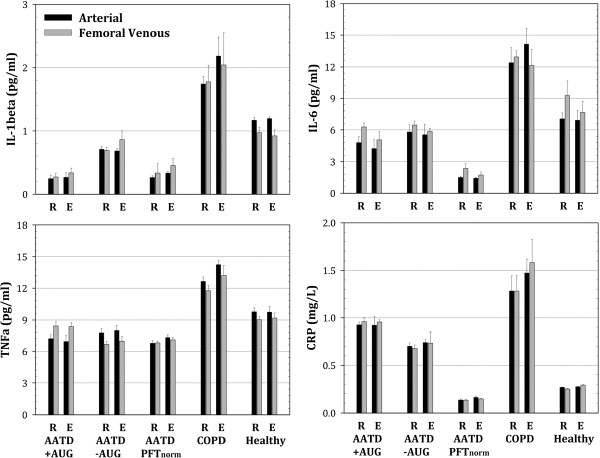
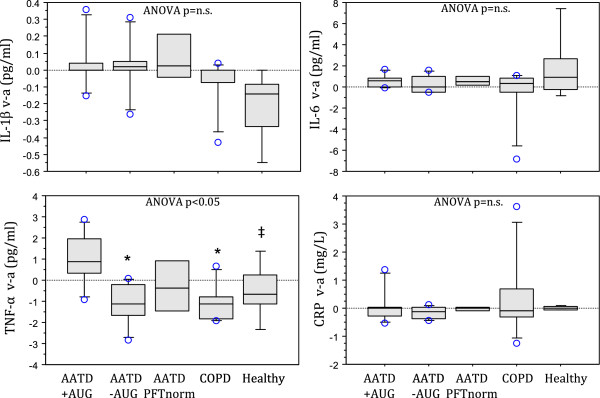
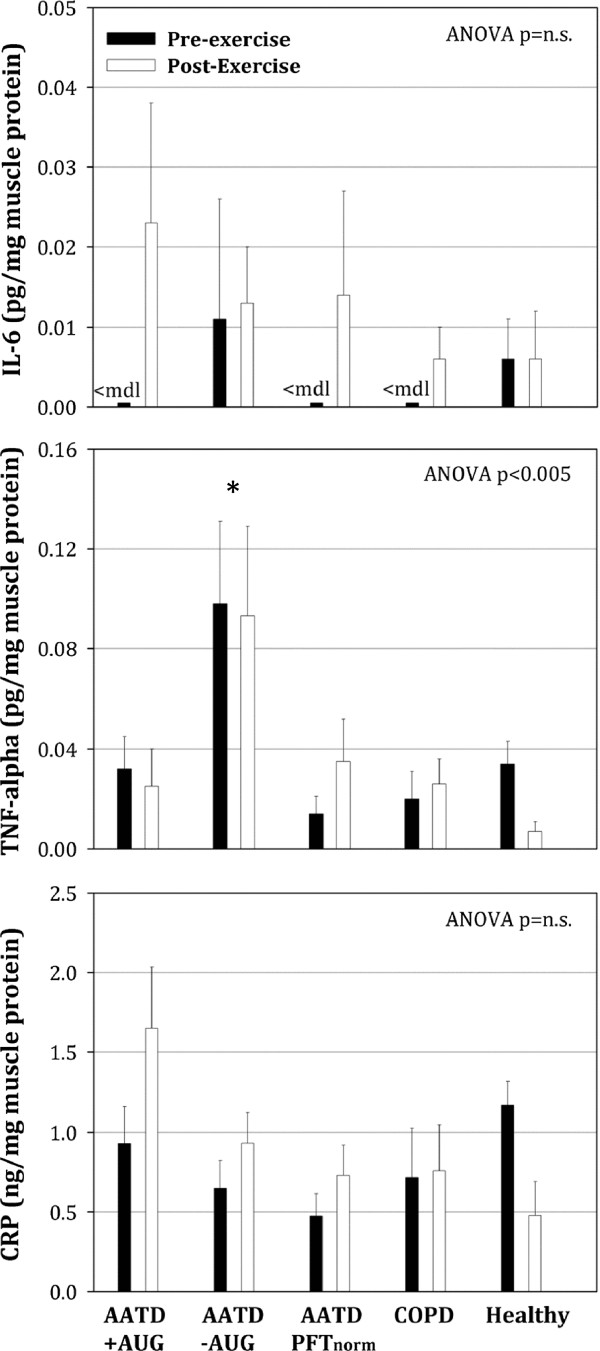
Circulating CRP was higher in AATD + AUG (4.7 ± 1.6 mg/dL) and AATD-AUG (3.3 ± 1.2 mg/dL) compared to healthy controls (1.5 ± 0.3 mg/dL, p < 0.05), but lower in AATD compared to non-AATD-COPD patients (6.1 ± 2.6 mg/dL, p < 0.05). TNFα, IL-6 and IL-1β were significantly increased by 1.7-, 1.7-, and 4.7-fold, respectively, in non-AATD COPD compared to AATD COPD (p < 0.05), and 1.3-, 1.7-, and 2.2-fold, respectively, compared to healthy subjects (p < 0.05). Skeletal muscle TNFα was on average 3-4 fold greater in AATD-AUG compared to the other groups (p < 0.05). Exercise showed no effect on these cytokines in any of our patient groups.
These data show that AATD COPD patients do not experience the same chronic systemic inflammation and exhibit reduced inflammation compared to non-AATD COPD patients. Augmentation therapy may help to improve muscle efflux of TNFα and reduce muscle TNFα concentration, but showed no effect on IL-6, IL-1β or CRP.
关于α-1抗胰蛋白酶缺乏症(AATD)慢性阻塞性肺疾病(COPD)患者的全身炎症,以及α-1抗胰蛋白酶补充疗法和/或运动对循环炎症细胞因子可能产生的影响,目前仍知之甚少。我们假设,接受补充疗法的AATD COPD患者(AATD + AUG)与未接受补充疗法的AATD COPD患者(AATD - AUG)和/或典型的非AATD(COPD)患者相比,其循环和骨骼肌炎症细胞因子水平会更低。我们还假设,与AATD - AUG或COPD受试者相比,AATD + AUG患者对运动的细胞因子反应会更低。
在所有COPD患者组中,包括另外两组(即肺功能正常的AATD患者和年龄/活动相匹配的健康对照组),于静息状态、50%最大1小时伸膝运动期间及运动后4小时,测量动脉和股静脉中肿瘤坏死因子α(TNFα)、白细胞介素-6(IL-6)、白细胞介素-1β(IL-1β)和C反应蛋白(CRP)的浓度以及骨骼肌中的表达。
与健康对照组(1.5±0.3mg/dL,p<0.05)相比,AATD + AUG组(4.7±1.6mg/dL)和AATD - AUG组(3.3±1.2mg/dL)的循环CRP水平更高,但与非AATD - COPD患者(6.1±2.6mg/dL,p<0.05)相比,AATD组的CRP水平更低。与AATD COPD患者相比,非AATD COPD患者的TNFα、IL-6和IL-1β分别显著升高1.7倍、1.7倍和4.7倍(p<0.05);与健康受试者相比,分别升高1.3倍、1.7倍和2.2倍(p<0.05)。与其他组相比,AATD - AUG组的骨骼肌TNFα平均高3 - 4倍(p<0.05)。运动对我们任何患者组的这些细胞因子均无影响。
这些数据表明,与非AATD COPD患者相比,AATD COPD患者不存在相同程度的慢性全身炎症,且炎症反应有所减轻。补充疗法可能有助于改善TNFα的肌肉外流并降低肌肉TNFα浓度,但对IL-6、IL-1β或CRP无影响。