Adams Alyce S, Madden Jeanne M, Zhang Fang, Soumerai Stephen B, Gilden Dan, Griggs Jennifer, Trinacty Connie M, Bishop Christine, Ross-Degnan Dennis
*Division of Research, Kaiser Permanente, Oakland, CA †Department of Population Medicine, Harvard Pilgrim Health Care Institute and Harvard Medical School, Boston, MA ‡Jen Associates Inc., Cambridge, MA §Department of Internal Medicine, University of Michigan, Ann Arbor, MI ∥Kaiser Permanente Center for Health Research, Honolulu, HI ¶The Heller School for Social Policy and Management, Brandeis University, Waltham, MA.
Med Care. 2014 Aug;52(8):695-703. doi: 10.1097/MLR.0000000000000159.
The use of lipid-lowering agents is suboptimal among dual enrollees, particularly blacks.
To determine whether the removal of restrictive drug caps under Medicare Part D reduced racial differences among dual enrollees with diabetes.
An interrupted time series with comparison series design (ITS) cohort study.
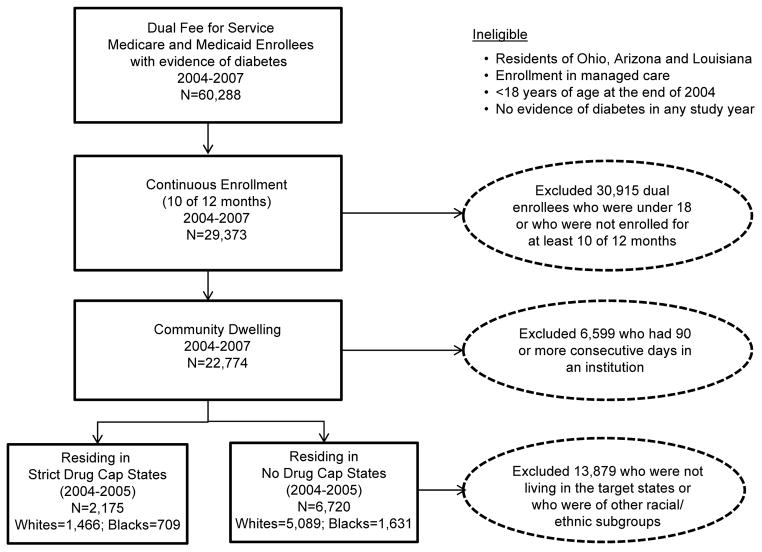
A total of 8895 black and white diabetes patients aged 18 years and older drawn from a nationally representative sample of fee-for-service dual enrollees (January 2004-December 2007) in states with and without drug caps before Part D.
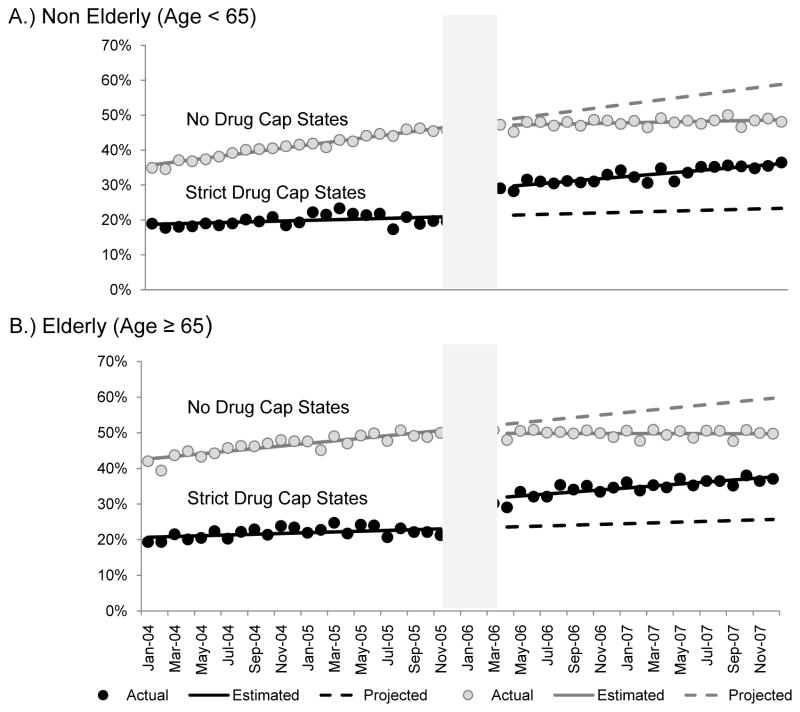
We examined the monthly (1) proportion of patients with any use of lipid-lowering therapies; and (2) intensity of use. Stratification measures included age (less than 65, 65 y and older), race (white vs. black), and sex.
At baseline, lipid-lowering drug use was higher in no drug cap states (drug cap: 54.0% vs. nondrug cap: 66.8%) and among whites versus blacks (drug cap: 58.5% vs. 44.9%, no drug cap: 68.4% vs. 61.9%). In strict drug cap states only, Part D was associated with an increase in the proportion with any use [nonelderly: +0.07 absolute percentage points (95% confidence interval, 0.06-0.09), P<0.001; elderly: +0.08 (0.06-0.10), P<0.001] regardless of race. However, we found no evidence of a change in the white-black gap in the proportion of users despite the removal of a significant financial barrier.
Medicare Part D was associated with increased use of lipid-lowering drugs, but racial gaps persisted. Understanding non-coverage-related barriers is critical in maximizing the potential benefits of coverage expansions for disparities reduction.
在双重参保者中,降脂药物的使用情况并不理想,尤其是黑人。
确定医疗保险D部分取消限制性药物上限是否减少了糖尿病双重参保者之间的种族差异。
一项带有对照系列设计的中断时间序列(ITS)队列研究。
从全国具有代表性的按服务收费的双重参保者样本(2004年1月至2007年12月)中选取了8895名18岁及以上的黑人和白人糖尿病患者,这些患者来自在D部分实施前有或没有药物上限的州。
我们检查了每月(1)使用任何降脂疗法的患者比例;以及(2)使用强度。分层指标包括年龄(小于65岁、65岁及以上)、种族(白人对黑人)和性别。
在基线时,无药物上限州的降脂药物使用率更高(有药物上限州:54.0%,无药物上限州:66.8%),白人的使用率高于黑人(有药物上限州:58.5%对44.9%,无药物上限州:68.4%对61.9%)。仅在严格实施药物上限的州,D部分与任何使用比例的增加相关[非老年人:绝对百分点增加0.07(95%置信区间,0.06 - 0.09),P < 0.001;老年人:增加0.08(0.06 - 0.10),P < 0.001],与种族无关。然而,尽管消除了重大的经济障碍,但我们没有发现使用者比例的黑白差距有变化的证据。
医疗保险D部分与降脂药物使用增加有关,但种族差距仍然存在。了解与未覆盖相关的障碍对于最大限度地扩大覆盖范围以减少差异的潜在益处至关重要。