Marques Elsa M R, Jones Hayley E, Elvers Karen T, Pyke Mark, Blom Ashley W, Beswick Andrew D
School of Social and Community Medicine, University of Bristol, Canynge Hall, 39 Whatley Road, Bristol BS8 2PS, UK.
BMC Musculoskelet Disord. 2014 Jul 5;15:220. doi: 10.1186/1471-2474-15-220.
Surgical pain is managed with multi-modal anaesthesia in total hip replacement (THR) and total knee replacement (TKR). It is unclear whether including local anaesthetic infiltration before wound closure provides additional pain control.
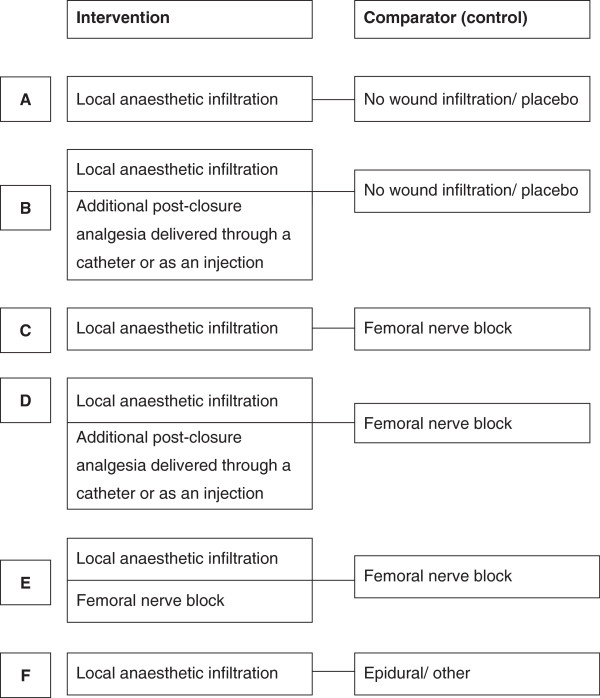
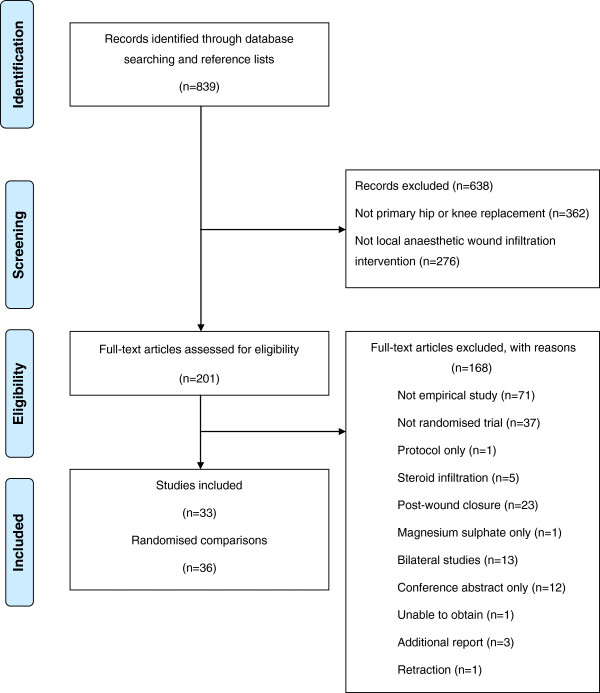
We performed a systematic review of randomised controlled trials of local anaesthetic infiltration in patients receiving THR or TKR. We searched MEDLINE, Embase and Cochrane CENTRAL to December 2012. Two reviewers screened abstracts, extracted data, and contacted authors for unpublished outcomes and data. Outcomes collected were post-operative pain at rest and during activity after 24 and 48 hours, opioid requirement, mobilisation, hospital stay and complications. When feasible, we estimated pooled treatment effects using random effects meta-analyses.
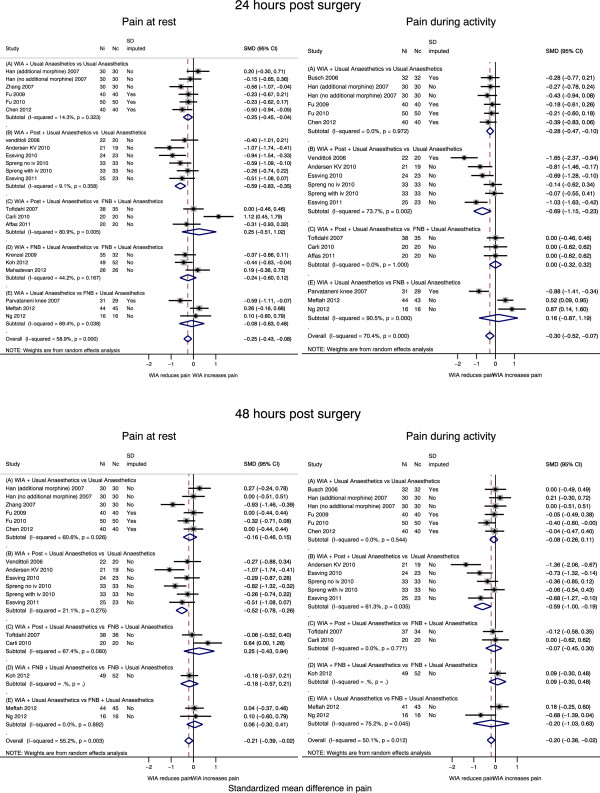
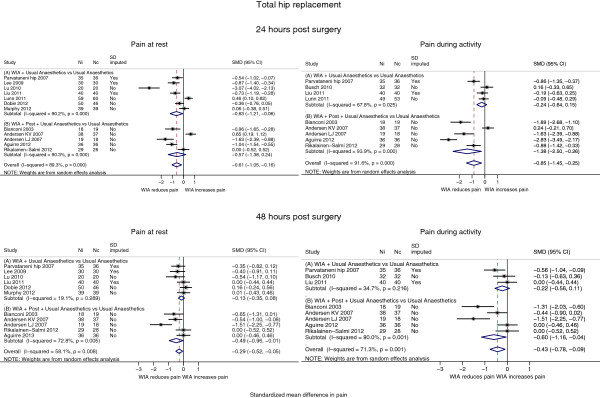
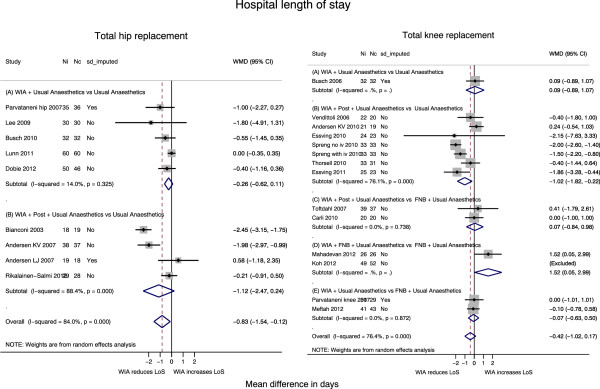
In 13 studies including 909 patients undergoing THR, patients receiving local anaesthetic infiltration experienced a greater reduction in pain at 24 hours at rest by standardised mean difference (SMD) -0.61 (95% CI -1.05, -0.16; p = 0.008) and by SMD -0.43 (95% CI -0.78 -0.09; p = 0.014) at 48 hours during activity.In TKR, diverse multi-modal regimens were reported. In 23 studies including 1439 patients undergoing TKR, local anaesthetic infiltration reduced pain on average by SMD -0.40 (95% CI -0.58, -0.22; p < 0.001) at 24 hours at rest and by SMD -0.27 (95% CI -0.50, -0.05; p = 0.018) at 48 hours during activity, compared with patients receiving no infiltration or placebo. There was evidence of a larger reduction in studies delivering additional local anaesthetic after wound closure. There was no evidence of pain control additional to that provided by femoral nerve block.Patients receiving local anaesthetic infiltration spent on average an estimated 0.83 (95% CI 1.54, 0.12; p = 0.022) and 0.87 (95% CI 1.62, 0.11; p = 0.025) fewer days in hospital after THR and TKR respectively, had reduced opioid consumption, earlier mobilisation, and lower incidence of vomiting.Few studies reported long-term outcomes.
Local anaesthetic infiltration is effective in reducing short-term pain and hospital stay in patients receiving THR and TKR. Studies should assess whether local anaesthetic infiltration can prevent long-term pain. Enhanced pain control with additional analgesia through a catheter should be weighed against a possible infection risk.
全髋关节置换术(THR)和全膝关节置换术(TKR)中的手术疼痛采用多模式麻醉进行管理。目前尚不清楚在伤口闭合前进行局部麻醉剂浸润是否能提供额外的疼痛控制。
我们对接受THR或TKR患者的局部麻醉剂浸润随机对照试验进行了系统评价。检索了截至2012年12月的MEDLINE、Embase和Cochrane CENTRAL。两名评价者筛选摘要、提取数据,并联系作者获取未发表的结果和数据。收集的结果包括术后24小时和48小时静息及活动时的疼痛、阿片类药物需求量、活动能力、住院时间和并发症。在可行的情况下,我们使用随机效应荟萃分析估计合并治疗效果。
在13项研究中,包括909例接受THR的患者,接受局部麻醉剂浸润的患者在24小时静息时疼痛减轻更明显,标准化均数差(SMD)为-0.61(95%CI -1.05,-0.16;p = 0.008),48小时活动时SMD为-0.43(95%CI -0.78,-0.09;p = 0.014)。在TKR中,报告了多种多模式方案。在23项研究中,包括1439例接受TKR的患者,与未接受浸润或安慰剂的患者相比,局部麻醉剂浸润在24小时静息时平均使疼痛减轻SMD -0.40(95%CI -0.58,-0.22;p < 0.001),48小时活动时SMD为-0.27(95%CI -0.50,-0.05;p = 0.018)。有证据表明,在伤口闭合后给予额外局部麻醉剂的研究中疼痛减轻幅度更大。没有证据表明除股神经阻滞提供的疼痛控制外还有额外的疼痛控制效果。接受局部麻醉剂浸润的患者在THR和TKR后平均住院天数分别减少0.83天(95%CI 1.54,0.12;p = 0.022)和0.87天(95%CI 1.62,0.11;p = 0.025),阿片类药物消耗量减少,活动更早,呕吐发生率更低。很少有研究报告长期结果。
局部麻醉剂浸润可有效减轻接受THR和TKR患者的短期疼痛并缩短住院时间。研究应评估局部麻醉剂浸润是否能预防长期疼痛。通过导管给予额外镇痛以增强疼痛控制应权衡可能的感染风险。