Bhargava Madhavi, Cajas Jorge Martinez, Wainberg Mark A, Klein Marina B, Pant Pai Nitika
Division of Clinical Epidemiology & Infectious Diseases, McGill University Health Centre, Montreal, Canada.
Division of Infectious Diseases, Department of Medicine, Queen's University, Kingston, Canada.
J Int AIDS Soc. 2014 Jul 4;17(1):18944. doi: 10.7448/IAS.17.1.18944. eCollection 2014.
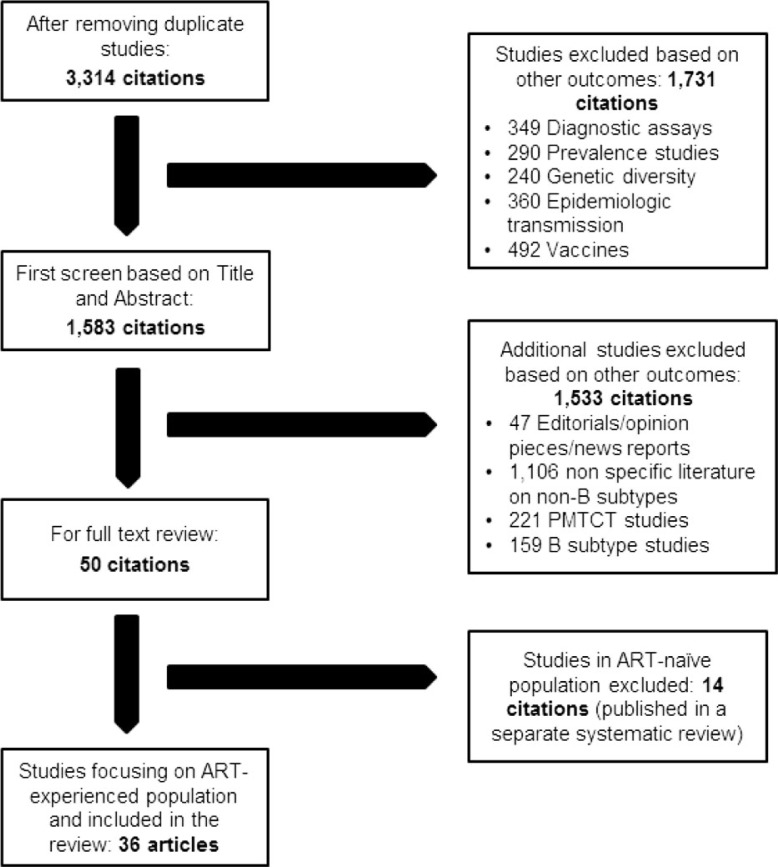
There are 31 million adults living with HIV-1 non-B subtypes globally, and about 10 million are on antiretroviral therapy (ART). Global evidence to guide clinical practice on ART response in HIV-1 non-B subtypes remains limited. We systematically searched 11 databases for the period 1996 to 2013 for evidence. Outcomes documented included time to development of AIDS and/or death, resistance mutations, opportunistic infections, and changes in CD4 cell counts and viral load. A lack of consistent reporting of all clinical end points precluded a meta-analysis. In sum, genetic diversity that precipitated differences in disease progression in ART-naïve populations was minimized in ART-experienced populations, although variability in resistance mutations persisted across non-B subtypes. To improve the quality of patient care in global settings, recording HIV genotypes at baseline and at virologic failure with targeted non-B subtype-based point-of-care resistance assays and timely phasing out of resistance-inducing ART regimens is recommended.
全球有3100万成年人感染HIV-1非B亚型,其中约1000万人正在接受抗逆转录病毒治疗(ART)。指导HIV-1非B亚型患者ART反应临床实践的全球证据仍然有限。我们系统检索了1996年至2013年期间的11个数据库以获取证据。记录的结果包括发展为艾滋病和/或死亡的时间、耐药突变、机会性感染以及CD4细胞计数和病毒载量的变化。由于缺乏对所有临床终点的一致报告,无法进行荟萃分析。总之,在初治人群中导致疾病进展差异的基因多样性在经治人群中最小化,尽管耐药突变在非B亚型之间仍存在差异。为了提高全球范围内的患者护理质量,建议在基线和病毒学失败时使用基于非B亚型的即时耐药检测记录HIV基因型,并及时淘汰诱导耐药的ART方案。