Department of Surgery and the Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
Departments of Health Policy, Management and Epidemiology, Johns Hopkins Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, USA.
BMJ. 2014 Jul 8;349:g4198. doi: 10.1136/bmj.g4198.
To determine casemix adjusted hospital level utilization of minimally invasive surgery for four common surgical procedures (appendectomy, colectomy, total abdominal hysterectomy, and lung lobectomy) in the United States.
Retrospective review.
United States.
Nationwide inpatient sample database, United States 2010.
For each procedure, a propensity score model was used to calculate the predicted proportion of minimally invasive operations for each hospital based on patient characteristics. For each procedure, hospitals were categorized into thirds (low, medium, and high) based on their actual to predicted proportion of utilization of minimally invasive surgery.
The primary outcome measures were the actual and predicted proportion of procedures performed with minimally invasive surgery. Secondary outcome measures included surgical complications and hospital characteristics.
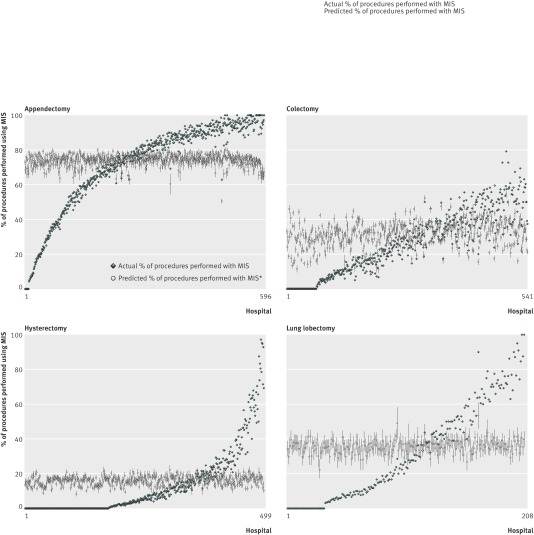
Mean hospital utilization of minimally invasive surgery was 71.0% (423/596) for appendectomy (range 40.9-93.1% (244-555)), 28.4% (154/541) for colectomy (6.7-49.8% (36/541-269/541)), 13.0% (65/499) for hysterectomy (0.0-33.6% (0/499-168/499)), and 32.0% (67/208) for lung lobectomy (3.6-65.7% (7.5/208-137/208)). Utilization of minimally invasive surgery was highly variable for each procedure type. There was noticeable discordance between actual and predicted utilization of the surgery (range of actual to predicted ratio for appendectomy 0-1.49; colectomy 0-3.88; hysterectomy 0-6.68; lung lobectomy 0-2.51). Surgical complications were less common with minimally invasive surgery compared with open surgery, respectively: overall rate for appendectomy 3.94% (1439/36,513) v 7.90% (958/12,123), P<0.001; for colectomy: 13.8% (1689/12,242) v 35.8% (8837/24,687), P<0.001; for hysterectomy: 4.69% (270/5757) v 6.64% (1988/29,940), P<0.001; and for lung lobectomy: 17.1% (367/2145) v 25.4% (971/3824), P<0.05. High utilization of minimally invasive surgery was associated with urban location (appendectomy: odds ratio 4.66, 95% confidence interval 1.17 to 18.5; colectomy: 4.59, 1.04 to 20.3; hysterectomy: 15.0, 2.98 to 75.0), large hospital size (hysterectomy: 8.70, 1.62 to 46.8), teaching hospital (hysterectomy: 5.41, 1.27 to 23.1), Midwest region (appendectomy: 7.85, 1.26 to 49.1), south region (appendectomy: 21.0, 3.79 to 117; colectomy: 10.0, 1.83 to 54.7), and west region (appendectomy: 9.33, 1.48 to 58.8).
Hospital utilization of minimally invasive surgery for appendectomy, colectomy, total abdominal hysterectomy, and lung lobectomy varies widely in the United States, representing a disparity in the surgical care delivered nationwide.
在美国确定四种常见手术(阑尾切除术、结肠切除术、全子宫切除术和肺叶切除术)微创手术的病例组合调整后的医院利用情况。
回顾性研究。
美国。
美国 2010 年全国住院患者样本数据库。
对于每种手术,使用倾向评分模型根据患者特征计算每个医院微创手术的预测比例。对于每种手术,根据实际与预测微创手术利用率的比例,将医院分为三分之一(低、中、高)。
主要观察指标是手术采用微创手术的实际和预测比例。次要观察指标包括手术并发症和医院特征。
阑尾切除术(范围 40.9%-93.1%(244-555))的平均微创手术利用率为 71.0%(423/596),结肠切除术(范围 6.7%-49.8%(36/541-269/541))为 28.4%(154/541),子宫切除术(范围 0.0%-33.6%(0/499-168/499))为 13.0%(65/499),肺叶切除术(范围 3.6%-65.7%(7.5/208-137/208))为 32.0%(67/208)。每种手术类型的微创手术利用率差异很大。实际与预测手术利用率之间存在明显差异(阑尾切除术范围为实际与预测比值 0-1.49;结肠切除术范围为 0-3.88;子宫切除术范围为 0-6.68;肺叶切除术范围为 0-2.51)。与开放式手术相比,微创手术的手术并发症较少,分别为:阑尾切除术的总体发生率为 3.94%(1439/36513)比 7.90%(958/12123),P<0.001;结肠切除术:13.8%(1689/12242)比 35.8%(8837/24687),P<0.001;子宫切除术:4.69%(270/5757)比 6.64%(1988/29940),P<0.001;肺叶切除术:17.1%(367/2145)比 25.4%(971/3824),P<0.05。微创手术的高利用率与城市位置(阑尾切除术:优势比 4.66,95%置信区间 1.17 至 18.5;结肠切除术:4.59,1.04 至 20.3;子宫切除术:15.0,2.98 至 75.0)、医院规模较大(子宫切除术:8.70,1.62 至 46.8)、教学医院(子宫切除术:5.41,1.27 至 23.1)、中西部地区(阑尾切除术:7.85,1.26 至 49.1)、南部地区(阑尾切除术:21.0,3.79 至 117;结肠切除术:10.0,1.83 至 54.7)和西部地区(阑尾切除术:9.33,1.48 至 58.8)有关。
美国阑尾切除术、结肠切除术、全子宫切除术和肺叶切除术的微创手术的医院利用情况差异很大,表明全国范围内提供的手术护理存在差异。