Alves Joao Guilherme B, de Araújo Carla Adriane Fonseca Leal, Pontes Isabelle E A, Guimarães Angélica C, Ray Joel G
Departments of Medicine, Obstetrics and Health Policy Management Evaluation, University of Toronto, St, Michael's Hospital, 30 Bond Street, Toronto, ON M5B 1 W8, Canada.
BMC Pregnancy Childbirth. 2014 Jul 8;14:222. doi: 10.1186/1471-2393-14-222.
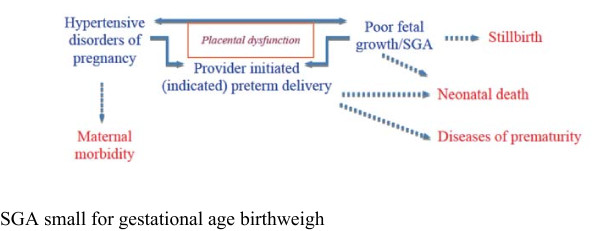
Preterm birth is the leading cause of infant mortality globally, including Brazil. We will evaluate whether oral magnesium citrate reduces the risk of placental dysfunction and its negative consequences for both the fetus and mother, which, in turn, should reduce the need for indicated preterm delivery.
METHODS/DESIGN: We will complete a multicenter, randomized double-blind clinical trial comparing oral magnesium citrate 150 mg twice daily (n = 2000 women) to matched placebo (n = 1000 women), starting at 121/7 to 206/7 weeks gestation and continued until delivery. We will include women at higher risk for placental dysfunction, based on clinical factors from a prior pregnancy (e.g., prior preterm delivery, stillbirth or preeclampsia) or the current pregnancy (e.g., chronic hypertension, pre-pregnancy diabetes mellitus, maternal age > 35 years or pre-pregnancy maternal body mass index > 30 kg/m2). The primary perinatal outcome is a composite of preterm birth < 37 weeks gestation, stillbirth > 20 weeks gestation, neonatal death < 28 days, or SGA birthweight < 3rd percentile. The primary composite maternal outcome is preeclampsia arising < 37 weeks gestation, severe non-proteinuric hypertension arising < 37 weeks gestation, placental abruption, maternal stroke during pregnancy or ≤ 7 days after delivery, or maternal death during pregnancy or ≤ 7 days after delivery.
The results of this randomized clinical trial may be especially relevant in low and middle income countries that have high rates of prematurity and limited resources for acute newborn and maternal care.
ClinicalTrials.gov Identifier NCT02032186, registered December 19, 2013.
早产是全球包括巴西在内婴儿死亡的主要原因。我们将评估口服枸橼酸镁是否能降低胎盘功能障碍的风险及其对胎儿和母亲的不良后果,进而减少因指征性早产的需求。
方法/设计:我们将完成一项多中心、随机双盲临床试验,比较每天两次口服150毫克枸橼酸镁(n = 2000名妇女)与匹配的安慰剂(n = 1000名妇女),从妊娠12 1/7至20 6/7周开始,持续至分娩。我们将纳入基于既往妊娠(如既往早产、死产或先兆子痫)或当前妊娠(如慢性高血压、孕前糖尿病、产妇年龄>35岁或孕前产妇体重指数>30kg/m²)的临床因素而有较高胎盘功能障碍风险的妇女。主要围产期结局是妊娠<37周早产、妊娠>20周死产、新生儿死亡<28天或小于胎龄儿出生体重<第3百分位数的综合指标。主要的产妇综合结局是妊娠<37周出现的先兆子痫、妊娠<37周出现的严重非蛋白尿性高血压、胎盘早剥、孕期或分娩后≤7天的产妇中风或孕期或分娩后≤7天的产妇死亡。
这项随机临床试验的结果在早产率高且急性新生儿和产妇护理资源有限的低收入和中等收入国家可能特别重要。
ClinicalTrials.gov标识符NCT02032186,于2013年12月19日注册。