Kye Bong-Hyeon, Kim Hyung-Jin, Kim Hyun-Sil, Kim Jun-Gi, Cho Hyeon-Min
1. St. Vincent Hospital, Department of Surgery, College of Medicine, The Catholic University of Korea, Suwon, Korea.
2. Seoul St. Mary's Hospital, Department of Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Int J Med Sci. 2014 Jun 9;11(9):857-62. doi: 10.7150/ijms.8874. eCollection 2014.
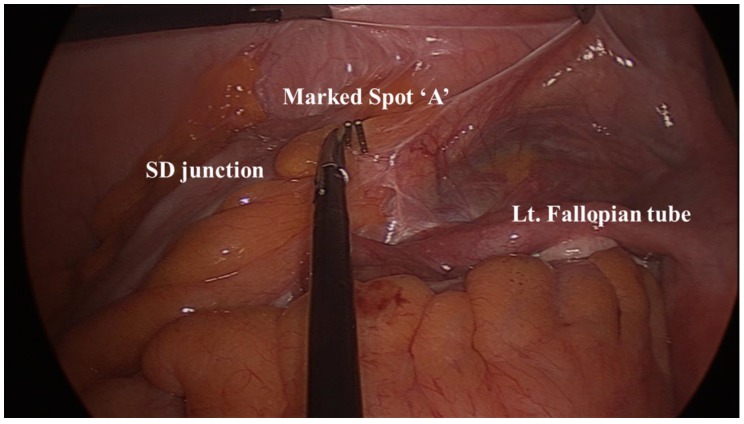
Splenic flexure mobilization (SFM) is performed to ensure a tension free anastomosis with an adequate resection margin in laparoscopic anterior resection (AR) or low anterior resection (LAR). This retrospective study was performed to determine the amount of colonic redundancy that can be expected by SFM.
Retrospective review of medical record for a total of 203 patients who underwent SFM during laparoscopic AR or LAR for the treatment of sigmoid colon or rectal cancer was performed.
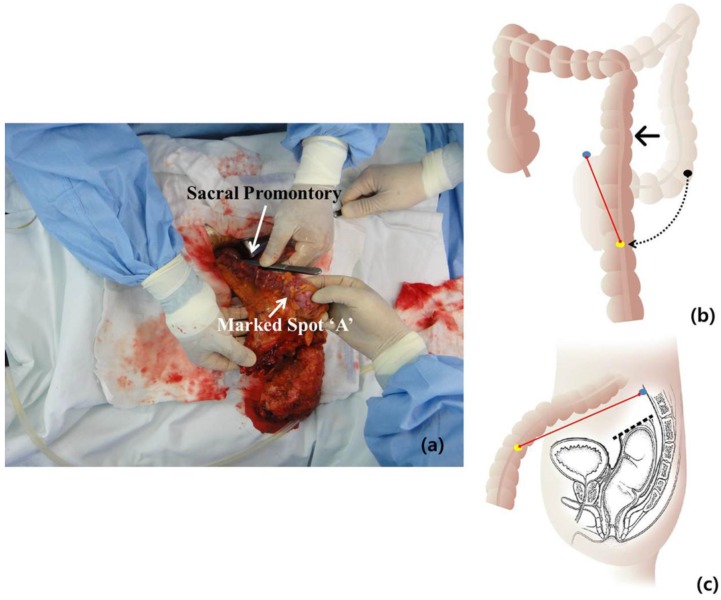
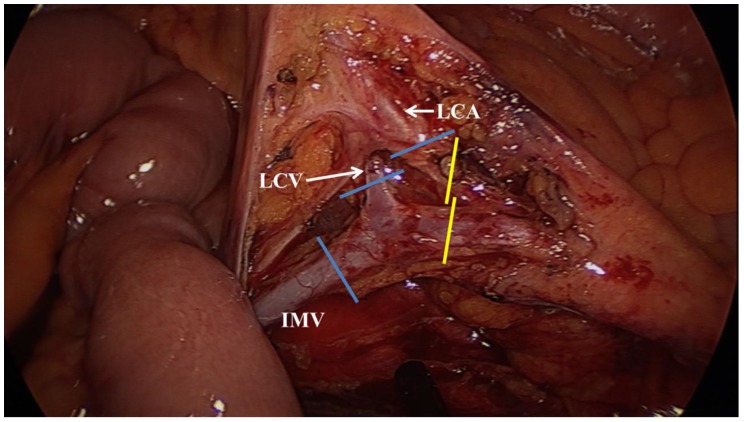
The obtained redundancy of the colon by SFM was 27.81 ± 7.29 cm from the sacral promontory. The redundancy of the colon by SFM with high ligation of the inferior mesenteric vein (IMV) (29.54 ± 7.17 cm from the sacral promontory) was greater than that with low ligation of the IMV (24.94 ± 6.07 cm from the sacral promontory, P < 0.0001). It took about 9.82% of the total operation time to perform SFM. There was no intraoperative complication during SFM.
SFM during laparoscopic AR or LAR is a safe and feasible option. Based on the result of this study, one can gain about 27.81 cm redundancy of the colon by SFM.
在腹腔镜前切除术(AR)或低位前切除术(LAR)中,进行脾曲游离(SFM)以确保无张力吻合并获得足够的切除边缘。本回顾性研究旨在确定通过SFM可预期的结肠冗余量。
对总共203例因乙状结肠癌或直肠癌在腹腔镜AR或LAR期间接受SFM的患者的病历进行回顾性分析。
通过SFM获得的结肠从骶岬起的冗余长度为27.81±7.29厘米。肠系膜下静脉(IMV)高位结扎的SFM所获得的结肠冗余(从骶岬起29.54±7.17厘米)大于IMV低位结扎的情况(从骶岬起24.94±6.07厘米,P<0.0001)。进行SFM约占总手术时间的9.82%。SFM期间无术中并发症。
腹腔镜AR或LAR期间的SFM是一种安全可行的选择。基于本研究结果,通过SFM可使结肠获得约27.81厘米的冗余。