Division of Digestive Surgery, University Hospitals of Geneva, Rue Gabrielle-Perret-Gentil 4, 1211, Geneva 14, Switzerland.
Medical School, University of Geneva, Rue Michel-Servet 1, 1206, Geneva, Switzerland.
Surg Endosc. 2023 Jul;37(7):5388-5396. doi: 10.1007/s00464-023-10008-x. Epub 2023 Apr 3.
Splenic flexure mobilization (SFM) may be indicated during anterior resection to provide a tension-free anastomosis. However, to date, no score allows identifying patients who may benefit from SFM.
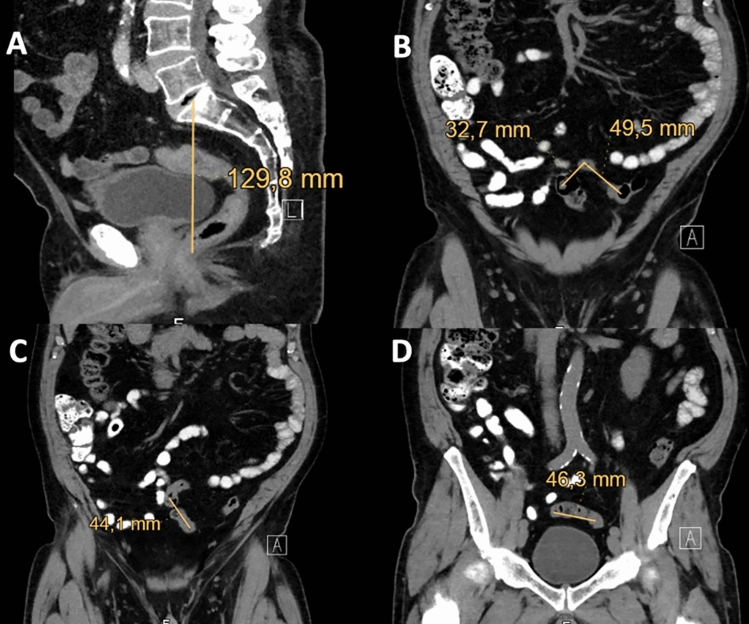
Patients who underwent robotic anterior resection for rectal cancer were identified from a prospective register. Demographic and cancer-related variables were extracted, and predictors of SFM were identified using regression models. Thereafter, 20 patients with SFM and 20 patients without SFM were randomly selected and their pre-operative CTscan were reviewed. The radiological index was defined as 1/(sigmoid length/pelvis depth). The optimal cut-off value for predicting SFM was identified using ROC curve analysis.
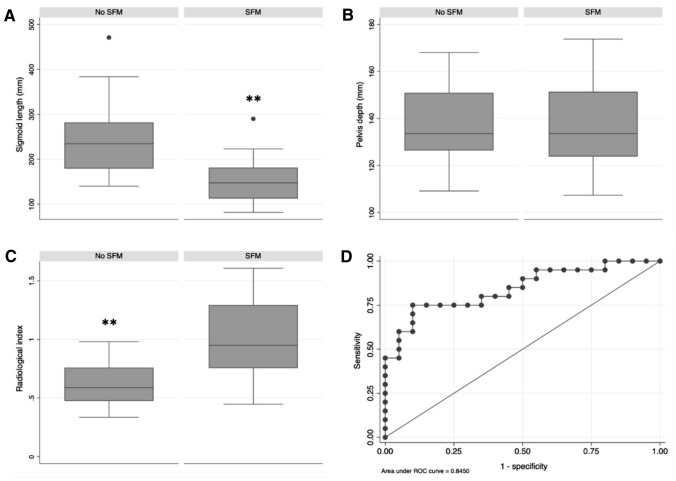
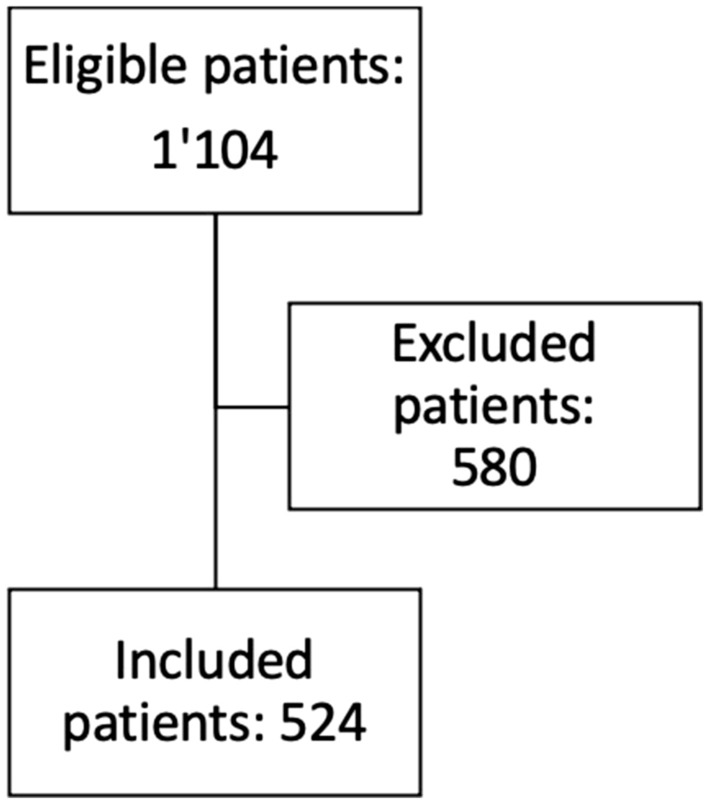
Five hundred and twenty-four patients were included. SFM was performed in 121 patients (27.8%) and increased operative time by 21.8 min (95% CI: 11.3 to 32.4, p < 0.001). The incidence of postoperative complications did not differ between patient with or without SFM. Realization of an anastomosis was the main predictor for SFM (OR: 42.4, 95% CI: 5.8 to 308.5, p < 0.001). In patients with colorectal anastomosis, both sigmoid length (15 ± 5.1 cm versus 24.2 ± 80.9 cm, p < 0.001) and radiological index (1 ± 0.3 versus 0.6 ± 0.2, p < 0.001) differed between patients who had SFM and patients who did not. ROC curve analysis of the radiological index indicated an optimal cut-off value of 0.8 (sensitivity: 75%, specificity: 90%).
SFM was performed in 27.8% of patients who underwent robotic anterior resection, and increased operative time by 21.8 min. For optimal surgical planning, patients requiring SFM can be identified based on pre-operative CT using the index 1/(sigmoid length/pelvis depth) with a cut-off value set at 0.8.
脾曲游离术(SFM)可能在直肠前切除术时使用,以提供无张力吻合。然而,到目前为止,还没有评分可以确定哪些患者可能受益于 SFM。
从前瞻性登记处确定接受机器人直肠前切除术的直肠癌患者。提取人口统计学和癌症相关变量,并使用回归模型确定 SFM 的预测因素。然后,随机选择 20 例接受 SFM 和 20 例未接受 SFM 的患者,并回顾其术前 CT 扫描。放射学指数定义为 1/(乙状结肠长度/骨盆深度)。使用 ROC 曲线分析确定预测 SFM 的最佳截断值。
共纳入 524 例患者。121 例(27.8%)患者行 SFM,手术时间延长 21.8 分钟(95%CI:11.3 至 32.4,p<0.001)。有或没有 SFM 的患者术后并发症发生率无差异。吻合的实现是 SFM 的主要预测因素(OR:42.4,95%CI:5.8 至 308.5,p<0.001)。在结直肠吻合患者中,SFM 患者的乙状结肠长度(15±5.1cm 与 24.2±80.9cm,p<0.001)和放射学指数(1±0.3 与 0.6±0.2,p<0.001)均与未行 SFM 的患者不同。放射学指数的 ROC 曲线分析表明,最佳截断值为 0.8(灵敏度:75%,特异性:90%)。
在接受机器人直肠前切除术的患者中,27.8%的患者行 SFM,手术时间延长 21.8 分钟。为了进行最佳的手术规划,可以使用术前 CT 基于指数 1/(乙状结肠长度/骨盆深度),并将截断值设置为 0.8,识别需要 SFM 的患者。