Wu Chen-Yi, Chou Yi-Chang, Huang Nicole, Chou Yiing-Jenq, Hu Hsiao-Yun, Li Chung-Pin
Institute of Public Health, National Yang Ming University, Taipei, Taiwan; Department of Dermatology, Taipei City Hospital, Heping Fuyou Branch, Taipei, Taiwan.
Institute of Public Health, National Yang Ming University, Taipei, Taiwan; Department of Education and Research, Taipei City Hospital, Taipei, Taiwan.
PLoS One. 2014 Jul 11;9(7):e102589. doi: 10.1371/journal.pone.0102589. eCollection 2014.
To evaluate the associations of body mass index (BMI) with all-cause, cardiovascular disease (CVD), and expanded CVD mortality in the elderly.
Observational cohort study.
Annual physical examination program for the elderly from 2006 to 2010.
We included 77,541 Taipei residents aged ≥ 65 years (39,365 men and 38,176 women).
BMI was categorized as underweight (BMI<18.5), normal weight (18.5 ≤ BMI<25), overweight (25 ≤ BMI<30), grade 1 obesity (30 ≤ BMI<35), or grade 2-3 obesity (BMI ≥ 35). Mortality was ascertained by national death files.
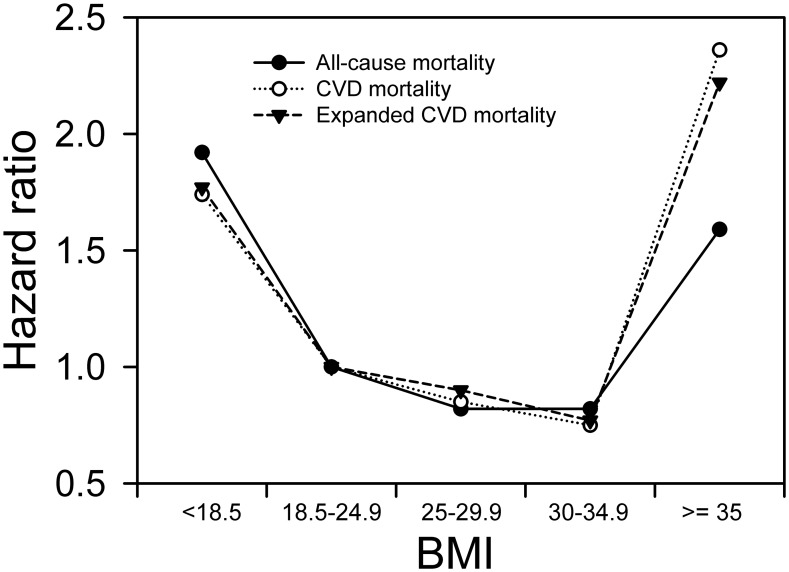
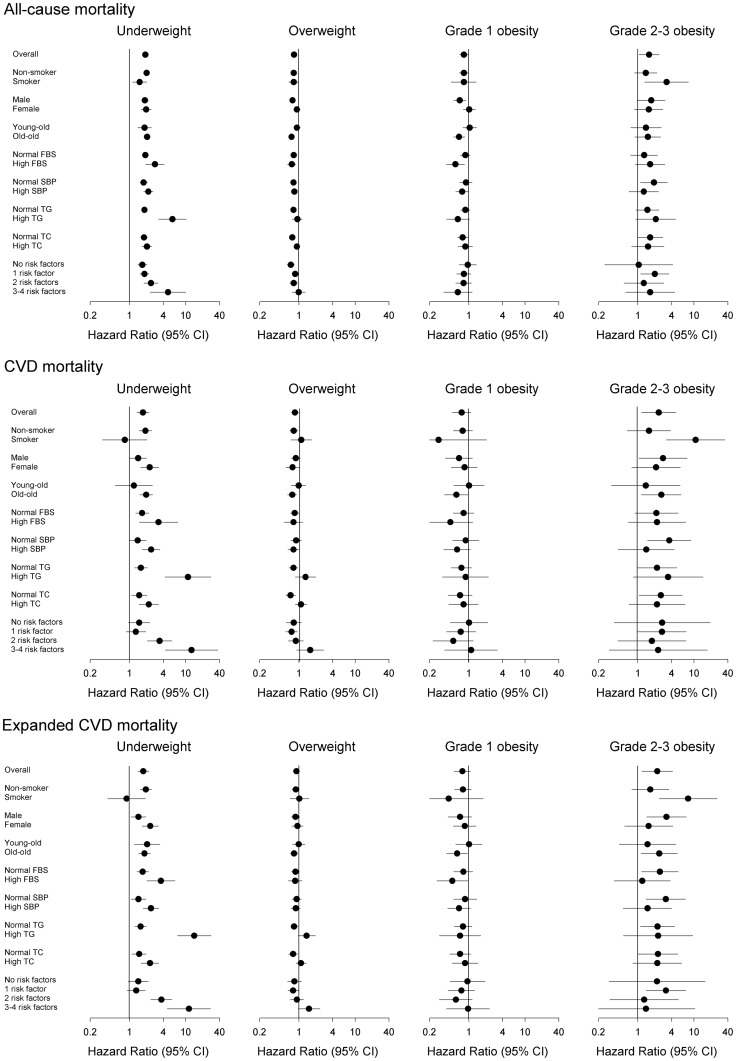
Underweight (hazard ratios [HRs] of all-cause, CVD, and expanded CVD mortality: 1.92, 1.74, and 1.77, respectively), grade 2-3 obesity (HRs: 1.59, 2.36, and 2.22, respectively), older age, male sex, smoking, and high fasting blood sugar were significant predictors of mortality. Meanwhile, being married/cohabitating, higher education, alcohol consumption, more regular exercise, and high total cholesterol were inversely associated with mortality. Multivariate stratified subgroup analyses verified smokers (HRs of all-cause, CVD, and expanded CVD mortality: 3.25, 10.71, and 7.86, respectively, for grade 2-3 obesity), the high triglyceride group (HRs: 5.82, 10.99, and 14.22, respectively for underweight), and patients with 3-4 factors related to metabolic syndrome (HRs: 4.86, 12.72, and 11.42, respectively, for underweight) were associated with mortality.
The associations of BMI with all-cause, CVD, expanded CVD mortality in the elderly are represented by U-shaped curves, suggesting unilateral promotions or interventions in weight reduction in the elderly may be inappropriate. Heterogeneous effects of grades 1 and 2-3 obesity on mortality were observed and should be treated as different levels of obesity.
评估老年人身体质量指数(BMI)与全因死亡率、心血管疾病(CVD)死亡率及扩展的CVD死亡率之间的关联。
观察性队列研究。
2006年至2010年老年人年度体检项目。
纳入77541名年龄≥65岁的台北居民(男性39365名,女性38176名)。
BMI分为体重过轻(BMI<18.5)、正常体重(18.5≤BMI<25)、超重(25≤BMI<30)、1级肥胖(30≤BMI<35)或2 - 3级肥胖(BMI≥35)。死亡率通过国家死亡档案确定。
体重过轻(全因死亡率、CVD死亡率及扩展的CVD死亡率的风险比[HRs]分别为1.92、1.74和1.77)、2 - 3级肥胖(HRs分别为1.59、2.36和2.22)、高龄、男性、吸烟及空腹血糖高是死亡率的显著预测因素。同时,已婚/同居、高学历、饮酒、规律运动较多及总胆固醇高与死亡率呈负相关。多变量分层亚组分析证实吸烟者(2 - 3级肥胖者的全因死亡率、CVD死亡率及扩展的CVD死亡率的HRs分别为3.25、10.71和7.86)、高甘油三酯组(体重过轻者的HRs分别为5.82、10.99和14.22)以及有3 - 4个与代谢综合征相关因素的患者(体重过轻者的HRs分别为4.86、12.72和11.42)与死亡率相关。
BMI与老年人全因死亡率、CVD死亡率及扩展的CVD死亡率之间的关联呈U形曲线,提示对老年人单方面提倡或干预减重可能不合适。观察到1级和2 - 3级肥胖对死亡率的异质性影响,应将其视为不同程度的肥胖。