DeVore Adam D, Hammill Bradley G, Sharma Puza P, Qualls Laura G, Mentz Robert J, Waltman Johnson Katherine, Fonarow Gregg C, Curtis Lesley H, Hernandez Adrian F
Duke Clinical Research Institute, Duke University School of Medicine, Durham, NC (A.D.D.V., B.G.H., L.G.Q., R.J.M., L.H.C., A.F.H.) Department of Medicine, Duke University School of Medicine, Durham, NC (A.D.D.V., R.J.M., L.H.C., A.F.H.).
Duke Clinical Research Institute, Duke University School of Medicine, Durham, NC (A.D.D.V., B.G.H., L.G.Q., R.J.M., L.H.C., A.F.H.).
J Am Heart Assoc. 2014 Jul 11;3(4):e001088. doi: 10.1161/JAHA.114.001088.
A subset of patients hospitalized with acute heart failure experiences worsening clinical status and requires escalation of therapy. Worsening heart failure is an end point in many clinical trials, but little is known about its prevalence in clinical practice and its associated outcomes.
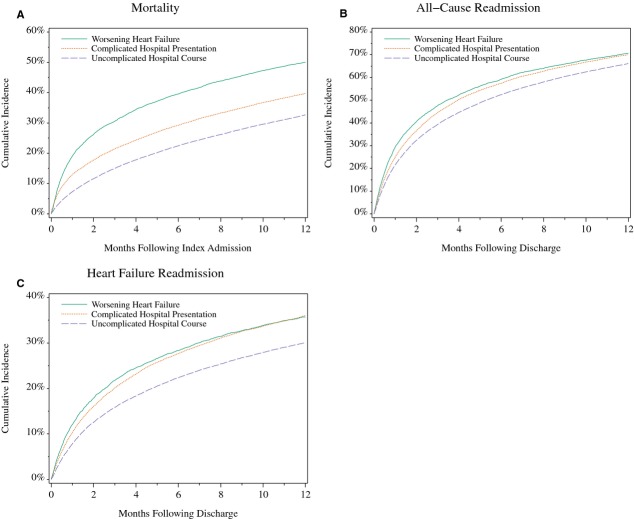
We analyzed inpatient data from the Acute Decompensated Heart Failure National Registry linked to Medicare claims to examine the prevalence and outcomes of patients with worsening heart failure, defined as the need for escalation of therapy at least 12 hours after hospital presentation. We compared patients with worsening heart failure to patients with an uncomplicated hospital course and patients with a complicated presentation. Of 63 727 patients hospitalized with acute heart failure, 11% developed worsening heart failure. These patients had the highest observed rates of mortality, all-cause readmission, and Medicare payments at 30 days and 1 year after hospitalization (P < 0.001 for all comparisons). The adjusted hazards of 30-day mortality were 2.56 (99% CI, 2.34 to 2.80) compared with an uncomplicated course and 1.29 (99% CI, 1.17 to 1.42) compared with a complicated presentation. The adjusted cost ratios for postdischarge Medicare payments at 30 days were 1.35 (99% CI, 1.24 to 1.46) compared with an uncomplicated course and 1.11 (99% CI, 1.02 to 1.22) compared with a complicated presentation.
In-hospital worsening heart failure was common and was associated with higher rates of mortality, all-cause readmission, and postdischarge Medicare payments. Prevention and treatment of in-hospital worsening heart failure represents an important goal for patients hospitalized with acute heart failure.
一部分因急性心力衰竭住院的患者临床状况会恶化,需要加强治疗。心力衰竭恶化是许多临床试验的终点,但对于其在临床实践中的患病率及其相关结局知之甚少。
我们分析了急性失代偿性心力衰竭国家注册数据库中与医疗保险理赔相关的住院患者数据,以研究心力衰竭恶化患者的患病率和结局,心力衰竭恶化定义为在入院至少12小时后需要加强治疗。我们将心力衰竭恶化患者与住院过程未出现并发症的患者以及入院时病情复杂的患者进行了比较。在63727例因急性心力衰竭住院的患者中,11%出现了心力衰竭恶化。这些患者在住院后30天和1年时的死亡率、全因再入院率和医疗保险支付率最高(所有比较的P<0.001)。与住院过程未出现并发症的患者相比,30天死亡率的校正风险比为2.56(99%CI,2.34至2.80);与入院时病情复杂的患者相比,校正风险比为1.29(99%CI,1.17至1.42)。与住院过程未出现并发症的患者相比,出院后30天医疗保险支付的校正成本比为1.35(99%CI,1.24至1.46);与入院时病情复杂的患者相比,校正成本比为1.11(99%CI,1.02至1.22)。
住院期间心力衰竭恶化很常见,且与更高的死亡率、全因再入院率以及出院后医疗保险支付率相关。预防和治疗住院期间心力衰竭恶化是急性心力衰竭住院患者的一个重要目标。