Wingfield Tom, Boccia Delia, Tovar Marco, Gavino Arquímedes, Zevallos Karine, Montoya Rosario, Lönnroth Knut, Evans Carlton A
Innovación Por la Salud Y Desarrollo (IPSYD), Asociación Benéfica PRISMA, Lima, Perú; Innovation For Health And Development (IFHAD), London, United Kingdom; Infectious Diseases & Immunity, Imperial College London, and Wellcome Trust Imperial College Centre for Global Health Research, London, United Kingdom; The Monsall Infectious Diseases Unit, North Manchester General Hospital, Manchester, United Kingdom.
Innovation For Health And Development (IFHAD), London, United Kingdom; Department of Infectious Disease Epidemiology, London School of Hygiene & Tropical Medicine, London, United Kingdom.
PLoS Med. 2014 Jul 15;11(7):e1001675. doi: 10.1371/journal.pmed.1001675. eCollection 2014 Jul.
Even when tuberculosis (TB) treatment is free, hidden costs incurred by patients and their households (TB-affected households) may worsen poverty and health. Extreme TB-associated costs have been termed "catastrophic" but are poorly defined. We studied TB-affected households' hidden costs and their association with adverse TB outcome to create a clinically relevant definition of catastrophic costs.
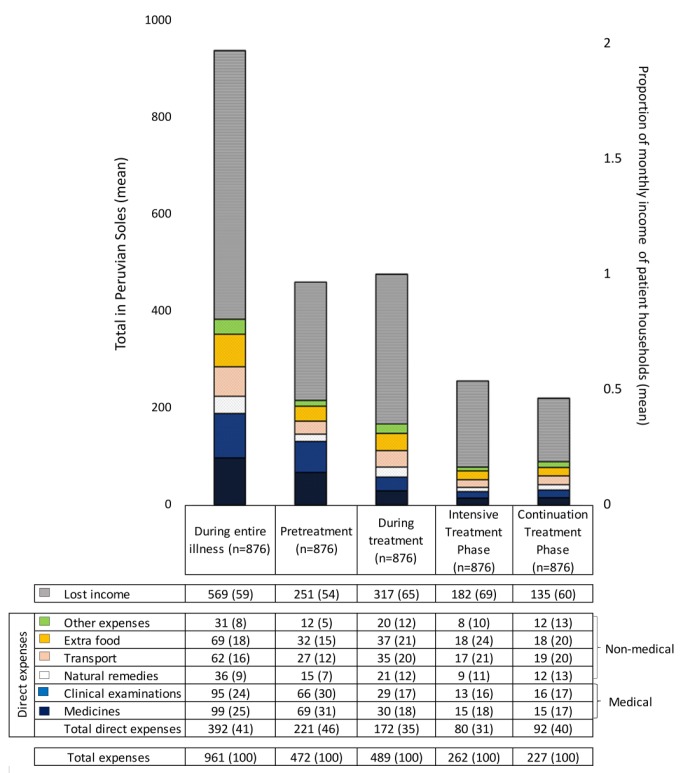
From 26 October 2002 to 30 November 2009, TB patients (n = 876, 11% with multi-drug-resistant [MDR] TB) and healthy controls (n = 487) were recruited to a prospective cohort study in shantytowns in Lima, Peru. Patients were interviewed prior to and every 2-4 wk throughout treatment, recording direct (household expenses) and indirect (lost income) TB-related costs. Costs were expressed as a proportion of the household's annual income. In poorer households, costs were lower but constituted a higher proportion of the household's annual income: 27% (95% CI = 20%-43%) in the least-poor houses versus 48% (95% CI = 36%-50%) in the poorest. Adverse TB outcome was defined as death, treatment abandonment or treatment failure during therapy, or recurrence within 2 y. 23% (166/725) of patients with a defined treatment outcome had an adverse outcome. Total costs ≥20% of household annual income was defined as catastrophic because this threshold was most strongly associated with adverse TB outcome. Catastrophic costs were incurred by 345 households (39%). Having MDR TB was associated with a higher likelihood of incurring catastrophic costs (54% [95% CI = 43%-61%] versus 38% [95% CI = 34%-41%], p<0.003). Adverse outcome was independently associated with MDR TB (odds ratio [OR] = 8.4 [95% CI = 4.7-15], p<0.001), previous TB (OR = 2.1 [95% CI = 1.3-3.5], p = 0.005), days too unwell to work pre-treatment (OR = 1.01 [95% CI = 1.00-1.01], p = 0.02), and catastrophic costs (OR = 1.7 [95% CI = 1.1-2.6], p = 0.01). The adjusted population attributable fraction of adverse outcomes explained by catastrophic costs was 18% (95% CI = 6.9%-28%), similar to that of MDR TB (20% [95% CI = 14%-25%]). Sensitivity analyses demonstrated that existing catastrophic costs thresholds (≥10% or ≥15% of household annual income) were not associated with adverse outcome in our setting. Study limitations included not measuring certain "dis-saving" variables (including selling household items) and gathering only 6 mo of costs-specific follow-up data for MDR TB patients.
Despite free TB care, having TB disease was expensive for impoverished TB patients in Peru. Incurring higher relative costs was associated with adverse TB outcome. The population attributable fraction indicated that catastrophic costs and MDR TB were associated with similar proportions of adverse outcomes. Thus TB is a socioeconomic as well as infectious problem, and TB control interventions should address both the economic and clinical aspects of this disease. Please see later in the article for the Editors' Summary.
即便结核病治疗是免费的,但患者及其家庭(受结核病影响的家庭)产生的隐性成本仍可能加剧贫困和健康问题。与结核病相关的极端成本被称为“灾难性”成本,但定义并不明确。我们研究了受结核病影响家庭的隐性成本及其与不良结核病结局的关联,以制定一个具有临床相关性的灾难性成本定义。
2002年10月26日至2009年11月30日,在秘鲁利马的棚户区开展了一项前瞻性队列研究,招募了结核病患者(n = 876,11%为耐多药结核病患者)和健康对照者(n = 487)。在治疗前及整个治疗过程中每2 - 4周对患者进行访谈,记录与结核病相关的直接成本(家庭支出)和间接成本(收入损失)。成本以家庭年收入的比例表示。在较贫困家庭中,成本较低,但占家庭年收入的比例较高:最不贫困家庭为27%(95%置信区间 = 20% - 43%),而最贫困家庭为48%(95%置信区间 = 36% - 50%)。不良结核病结局定义为治疗期间死亡、治疗中断或治疗失败,或在2年内复发。在有明确治疗结局的患者中,23%(166/725)出现了不良结局。家庭年收入总成本≥20%被定义为灾难性成本,因为该阈值与不良结核病结局关联最为紧密。345个家庭(39%)产生了灾难性成本。患有耐多药结核病的患者产生灾难性成本的可能性更高(54% [95%置信区间 = 43% - 61%] 对38% [95%置信区间 = 34% - 41%],p<0.003)。不良结局与耐多药结核病(比值比[OR] = 8.4 [95%置信区间 = 4.7 - 15],p<0.001)、既往结核病(OR = 2.1 [95%置信区间 = 1.3 - 3.5],p = 0.005)、治疗前因病无法工作的天数(OR = 1.01 [95%置信区间 = 1.00 - 1.01],p = 0.02)以及灾难性成本(OR = 1.7 [95%置信区间 = 1.1 - 2.6],p = 0.01)独立相关。灾难性成本所解释的不良结局的调整人群归因分数为18%(95%置信区间 = 6.9% - 28%),与耐多药结核病的情况相似(20% [95%置信区间 = 14% - 25%])。敏感性分析表明,在我们的研究环境中,现有的灾难性成本阈值(家庭年收入≥10%或≥15%)与不良结局无关。研究局限性包括未测量某些“负储蓄”变量(包括出售家庭物品),且仅收集了耐多药结核病患者6个月的特定成本随访数据。
尽管结核病护理是免费的,但对于秘鲁贫困的结核病患者来说,患结核病的成本很高。产生较高的相对成本与不良结核病结局相关。人群归因分数表明,灾难性成本和耐多药结核病与相似比例的不良结局相关。因此,结核病既是一个社会经济问题,也是一个传染病问题,结核病控制干预措施应同时解决该疾病的经济和临床方面的问题。请参阅本文后面的编辑总结。