Fransz Duncan P, Schönhuth Casper P, Postma Tjeerd J, van Royen Barend J
Department of Orthopaedic Surgery, VU University Medical Center, PO Box 7057, 1007 MB Amsterdam, The Netherlands.
BMC Musculoskelet Disord. 2014 Aug 7;15:265. doi: 10.1186/1471-2474-15-265.
The 'Parsonage-Turner syndrome' (PTS) is a rare but distinct disorder with an abrupt onset of shoulder pain, followed by weakness and atrophy of the upper extremity musculature, and a slow recovery requiring months to years. To our best knowledge, this is the first case describing symptoms and signs of PTS following the administration of a post-exposure prophylaxis (PEP) regimen against possible human immunodeficiency virus (HIV) and hepatitis B virus (HBV) infection.
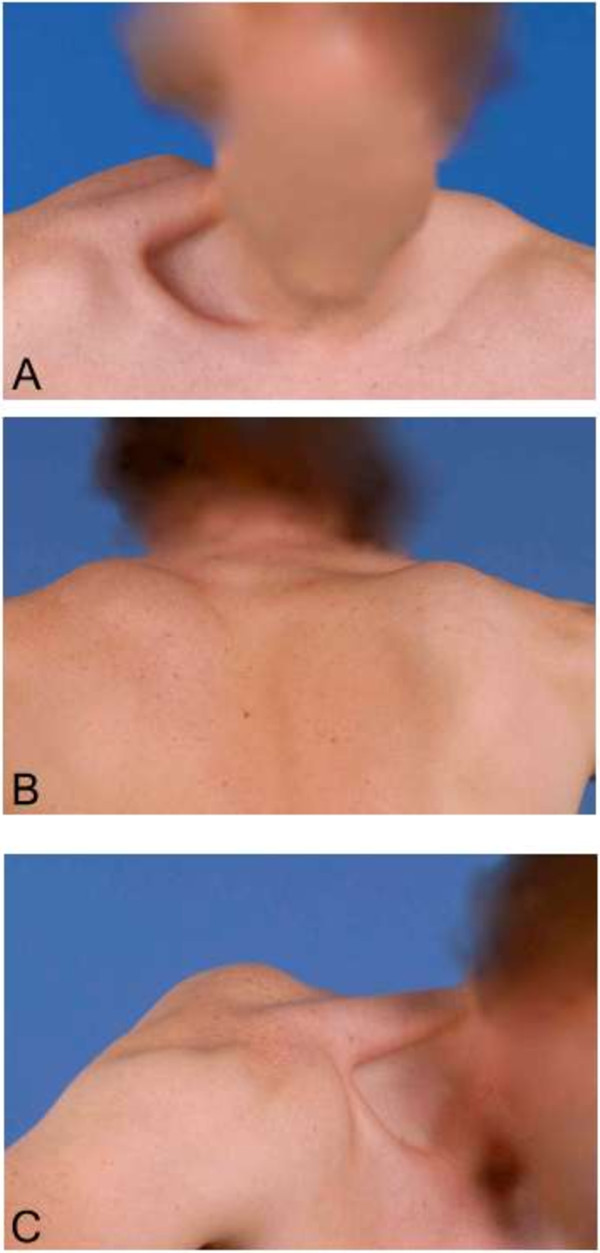
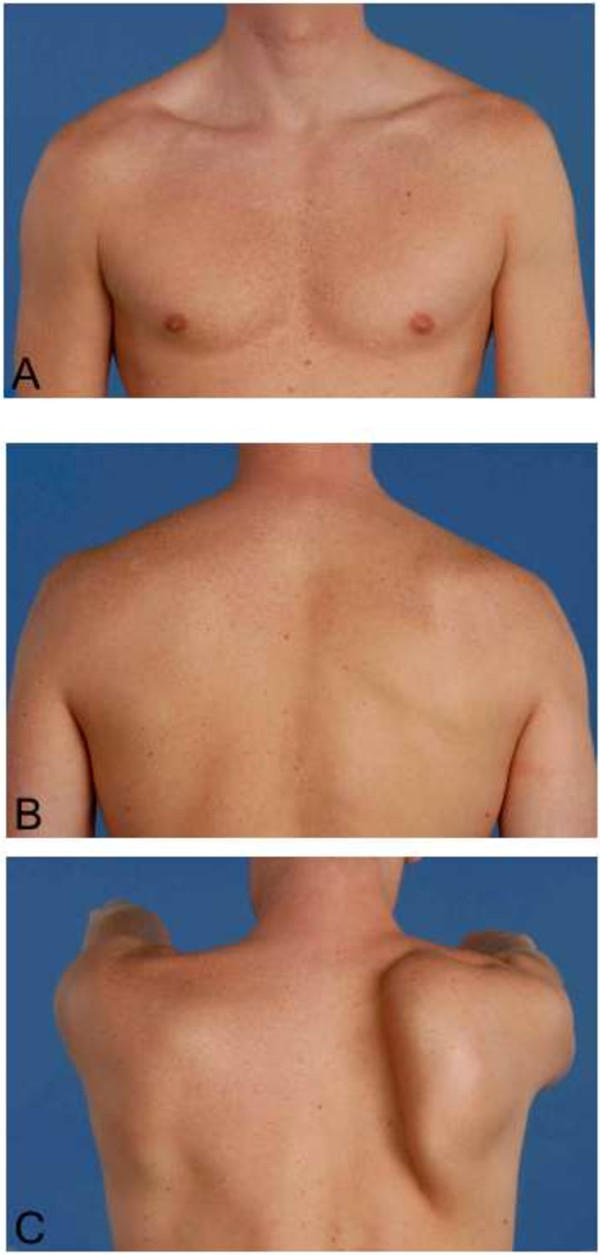
A 25-year-old Caucasian man presented with pain and unilateral scapular winging following PEP against possible HIV and HBV infection. Although atrophy and weakness were observed for the right supraspinatus muscle, a full range of motion was achievable. Neurological examination, plain radiography of the right shoulder and electromyography showed no additional abnormalities. The patient was diagnosed with post-vaccination PTS and treated non-operatively. During the following 15 months the scapular winging receded and full muscle strength was regained.
Parsonage-Turner syndrome is a rare clinical diagnosis. The precise pathophysiological mechanism of PTS remains unclear, but it seems to involve an interaction between genetic predisposition, mechanical vulnerability and an autoimmune trigger. An immunological event, such as - in this case - a vaccination as part of PEP treatment, can trigger the onset of PTS. The clinical presentation is distinctive with acute severe pain followed by patchy paresis, atrophy and sensory symptoms that persist for months to years. No currently available tests can provide a definite confirmation or exclusion of PTS. Routine blood examination, electromyography (EMG), and computed tomography (CT) or magnetic resonance imaging (MRI) serve mainly to exclude other disorders. The recovery can be quite lengthy, non-operative treatment is the accepted practice. Supplementary administration of oral prednisolone could shorten the duration of pain. Although the outcome is typically preferable, a substantial amount of patients are left with some residual paresis and functional impairment.
“Parsonage-Turner综合征”(PTS)是一种罕见但独特的疾病,起病急骤,表现为肩部疼痛,随后出现上肢肌肉无力和萎缩,恢复缓慢,需要数月至数年时间。据我们所知,这是首例描述在接受针对可能的人类免疫缺陷病毒(HIV)和乙型肝炎病毒(HBV)感染的暴露后预防(PEP)方案后出现PTS症状和体征的病例。
一名25岁的白人男性在接受针对可能的HIV和HBV感染的PEP后,出现疼痛和单侧肩胛翼状肩。虽然右侧冈上肌观察到萎缩和无力,但仍可实现全范围活动。神经学检查、右肩X线平片和肌电图均未显示其他异常。该患者被诊断为接种疫苗后PTS,并接受了非手术治疗。在接下来的15个月里,肩胛翼状肩逐渐减轻,肌肉力量完全恢复。
Parsonage-Turner综合征是一种罕见的临床诊断。PTS的确切病理生理机制尚不清楚,但似乎涉及遗传易感性、机械易损性和自身免疫触发因素之间的相互作用。免疫事件,如在本病例中作为PEP治疗一部分的疫苗接种,可触发PTS的发作。临床表现独特,先是急性剧痛,随后是散在性轻瘫、萎缩和感觉症状,持续数月至数年。目前尚无可用的检查能明确确诊或排除PTS。常规血液检查、肌电图(EMG)以及计算机断层扫描(CT)或磁共振成像(MRI)主要用于排除其他疾病。恢复过程可能相当漫长,非手术治疗是公认的做法。口服泼尼松龙辅助给药可缩短疼痛持续时间。尽管通常预后较好,但仍有相当数量的患者会遗留一些残余轻瘫和功能障碍。