Barnato Amber E, Cohen Elan D, Mistovich Keili A, Chang Chung-Chou H
Department of Medicine, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, USA; Department of Health Care Policy and Management, University of Pittsburgh Graduate School of Public Health, Pittsburgh, Pennsylvania, USA.
Department of Medicine, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, USA.
J Pain Symptom Manage. 2015 Mar;49(3):521-9.e1-5. doi: 10.1016/j.jpainsymman.2014.06.017. Epub 2014 Aug 15.
Hospitals vary substantially in their end-of-life (EOL) treatment intensity. It is unknown if patterns of EOL treatment intensity are consistent across conditions.
To explore the relationship between hospitals' cancer- and non-cancer-specific EOL treatment intensity.
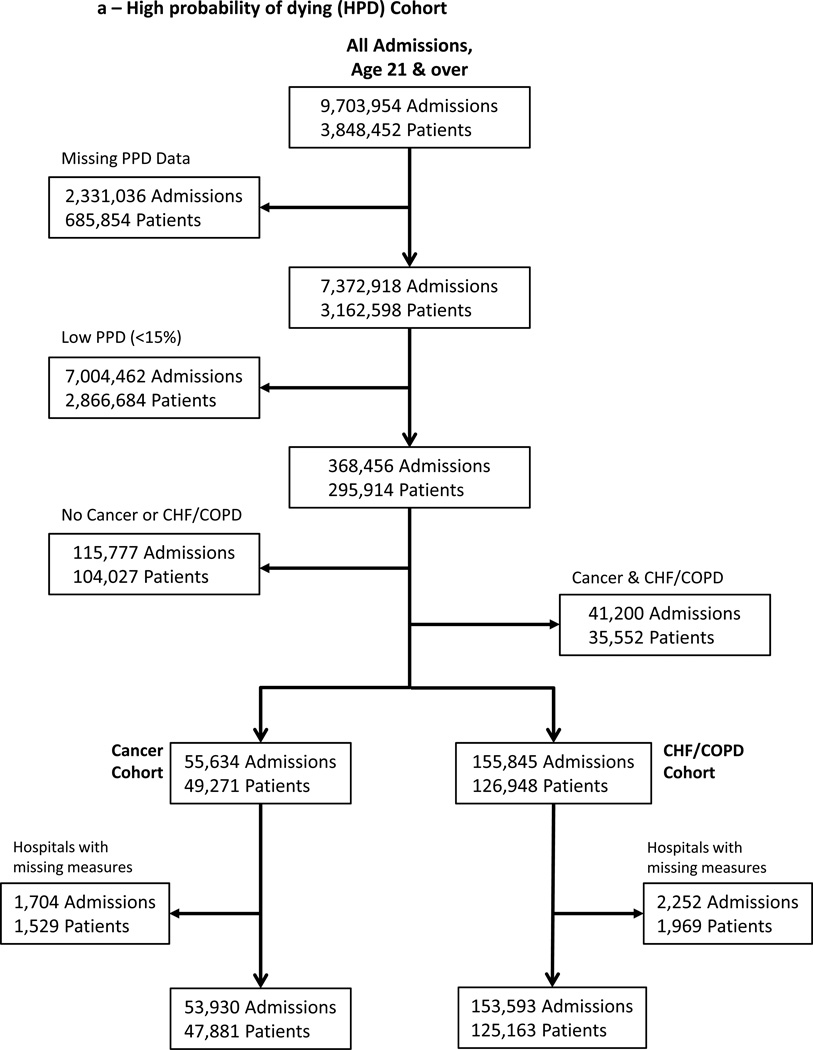
We conducted a retrospective cohort analysis of Pennsylvania acute care hospital admissions for either cancer or congestive heart failure (CHF) and/or chronic obstructive pulmonary disease (COPD) between 2001 and 2007, linked to vital statistics through 2008. We calculated Bayes's shrunken case-mix standardized (observed-to-expected) ratios of intensive care and life-sustaining treatment use among two EOL cohorts: those prospectively identified at high probability of dying on admission and those retrospectively identified as terminal admissions (decedents). We then summed these to create a hospital-specific prospective and retrospective overall EOL treatment intensity index for cancer vs. CHF/COPD.
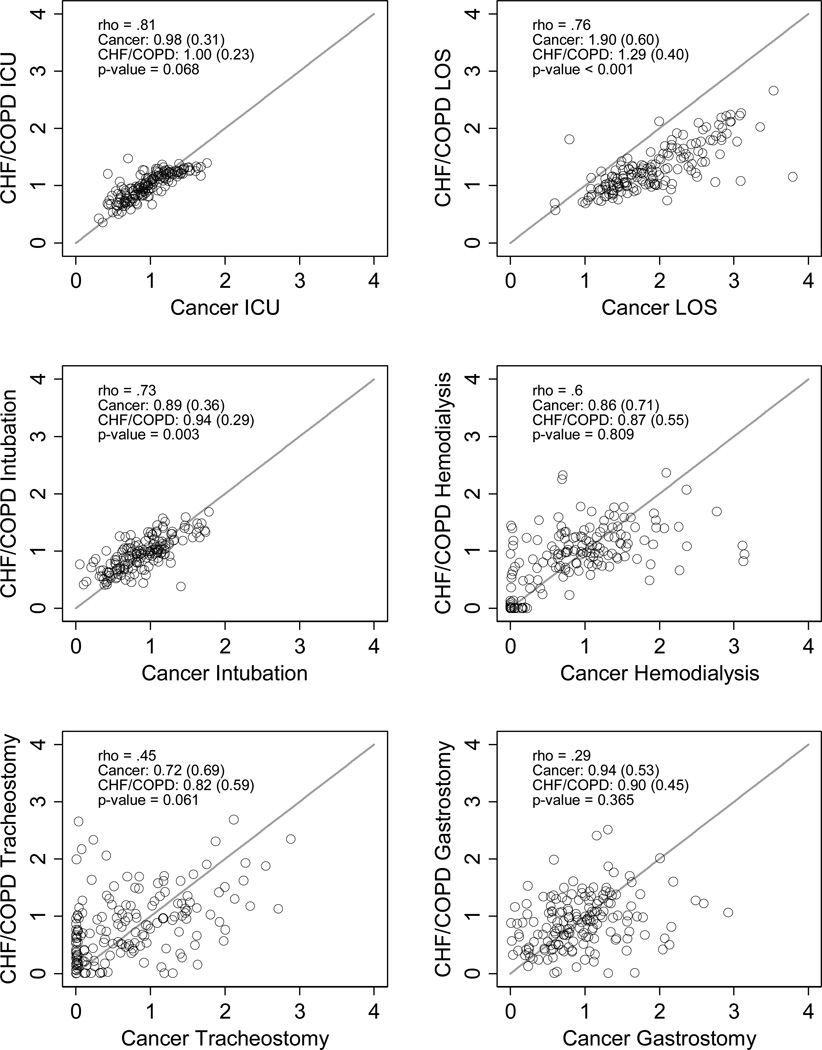
The sample included 207,523 admissions with 15% or greater predicted probability of dying on admission among 172,041 unique adults and 120,372 terminal admissions at 166 hospitals; these two cohorts overlapped by 52,986 admissions. There was substantial variation between hospitals in their standardized EOL treatment intensity ratios among cancer and CHF/COPD admissions. Within hospitals, cancer- and CHF/COPD-specific standardized EOL treatment intensity ratios were highly correlated for intensive care unit (ICU) admission (prospective ρ = 0.81; retrospective ρ = 0.78), ICU lengths of stay (ρ = 0.76; 0.64), mechanical ventilation (ρ = 0.73; 0.73), and hemodialysis (ρ = 0.60; 0.71) and less highly correlated for tracheostomy (ρ = 0.43; 0.53) and gastrostomy (ρ = 0.29; 0.30). Hospitals' overall EOL intensity index for cancer and CHF admissions were correlated (prospective ρ = 0.75; retrospective ρ = 0.75) and had equal group means (P-value = 0.631; 0.699).
Despite substantial difference between hospitals in EOL treatment intensity, within-hospital homogeneity in EOL treatment intensity for cancer- and non-cancer populations suggests the existence of condition-insensitive institutional norms of EOL treatment.
医院在临终(EOL)治疗强度方面差异很大。目前尚不清楚临终治疗强度模式在不同疾病中是否一致。
探讨医院针对癌症和非癌症的临终治疗强度之间的关系。
我们对2001年至2007年间宾夕法尼亚州急性护理医院收治的癌症患者或充血性心力衰竭(CHF)和/或慢性阻塞性肺疾病(COPD)患者进行了回顾性队列分析,并将其与截至2008年的生命统计数据相关联。我们计算了两个临终队列中重症监护和维持生命治疗使用情况的贝叶斯收缩病例组合标准化(观察值与预期值)比率:那些入院时被前瞻性确定为高死亡概率的患者以及那些被回顾性确定为末期入院(死者)的患者。然后,我们将这些比率相加,以创建针对癌症与CHF/COPD的特定医院前瞻性和回顾性总体临终治疗强度指数。
样本包括172,041名独特成年人中预测入院时死亡概率为15%或更高的207,523例入院病例,以及166家医院的120,372例末期入院病例;这两个队列有52,986例入院病例重叠。在癌症和CHF/COPD入院病例的标准化临终治疗强度比率方面,医院之间存在很大差异。在医院内部,针对癌症和CHF/COPD的标准化临终治疗强度比率在重症监护病房(ICU)入院方面高度相关(前瞻性ρ = 0.81;回顾性ρ = 0.78)、ICU住院时长(ρ = 0.76;0.64)、机械通气(ρ = 0.73;0.73)和血液透析(ρ = 0.60;0.71)方面相关性较高,而在气管切开术(ρ = 0.43;0.53)和胃造口术(ρ = 0.29;0.30)方面相关性较低。医院针对癌症和CHF入院的总体临终强度指数具有相关性(前瞻性ρ = 0.75;回顾性ρ = 0.75)且组均值相等(P值 = 0.631;0.699)。
尽管医院在临终治疗强度方面存在很大差异,但癌症和非癌症人群在医院内部临终治疗强度的同质性表明存在对疾病不敏感的临终治疗机构规范。