Chung Michael H, Beck Ingrid A, Dross Sandra, Tapia Kenneth, Kiarie James N, Richardson Barbra A, Overbaugh Julie, Sakr Samah R, John-Stewart Grace C, Frenkel Lisa M
Departments of *Global Health; †Medicine; ‡Epidemiology, University of Washington, Seattle, WA; §Center for Global Infectious Disease Research, Seattle Children's Research Institute, Seattle, WA; ‖Department of Obstetrics and Gynaecology, University of Nairobi, Nairobi, Kenya; ¶Department of Biostatistics, University of Washington, Seattle, WA; #Division of Public Health Sciences, Fred Hutchinson Cancer Research Center, Seattle, WA; **Division of Human Biology, Fred Hutchinson Cancer Research Center, Seattle, WA; ††Coptic Hospital, Nairobi, Kenya; Departments of ‡‡Pediatrics; and §§Laboratory Medicine, University of Washington, Seattle, WA.
J Acquir Immune Defic Syndr. 2014 Nov 1;67(3):246-53. doi: 10.1097/QAI.0000000000000312.
Transmitted drug resistance (TDR) is increasing in some areas of Africa. Detection of TDR may predict virologic failure of first-line nonnucleoside reverse transcriptase inhibitor (NNRTI)-based antiretroviral therapy (ART). We evaluated the utility of a relatively inexpensive oligonucleotide ligation assay (OLA) to detect clinically relevant TDR at the time of ART initiation.
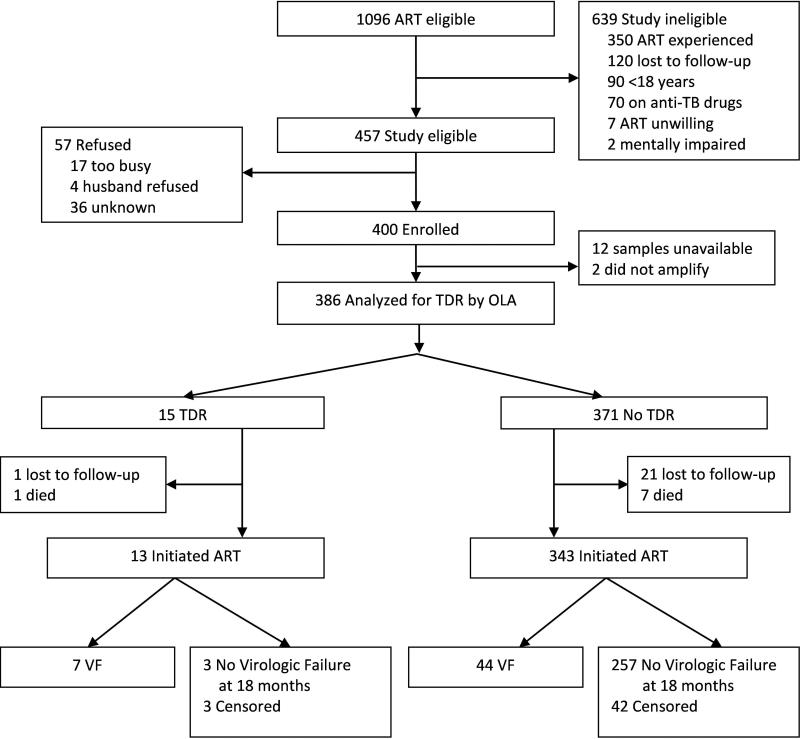
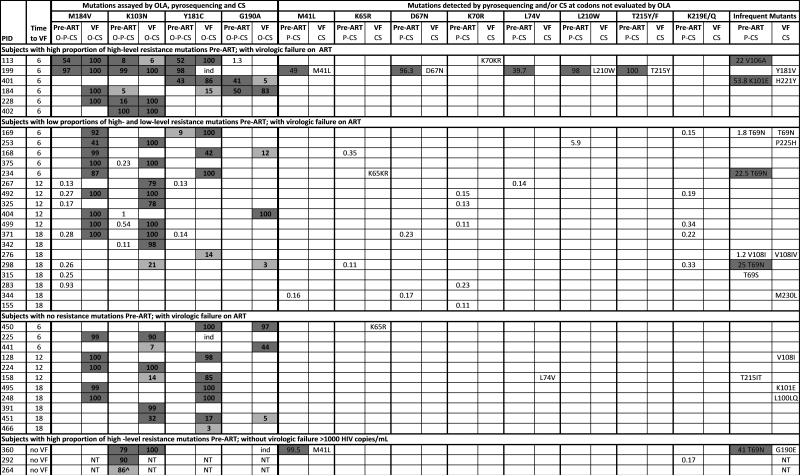
Pre-ART plasmas from ART-naive Kenyans initiating an NNRTI-based fixed-dose combination ART in a randomized adherence trial conducted in 2006 were retrospectively analyzed by OLA for mutations conferring resistance to NNRTI (K103N, Y181C, and G190A) and lamivudine (M184V). Post-ART plasmas were analyzed for virologic failure (≥1000 copies/mL) at 6-month intervals over 18-month follow-up. Pre-ART plasmas of those with virologic failure were evaluated for drug resistance by consensus and 454-pyrosequencing.
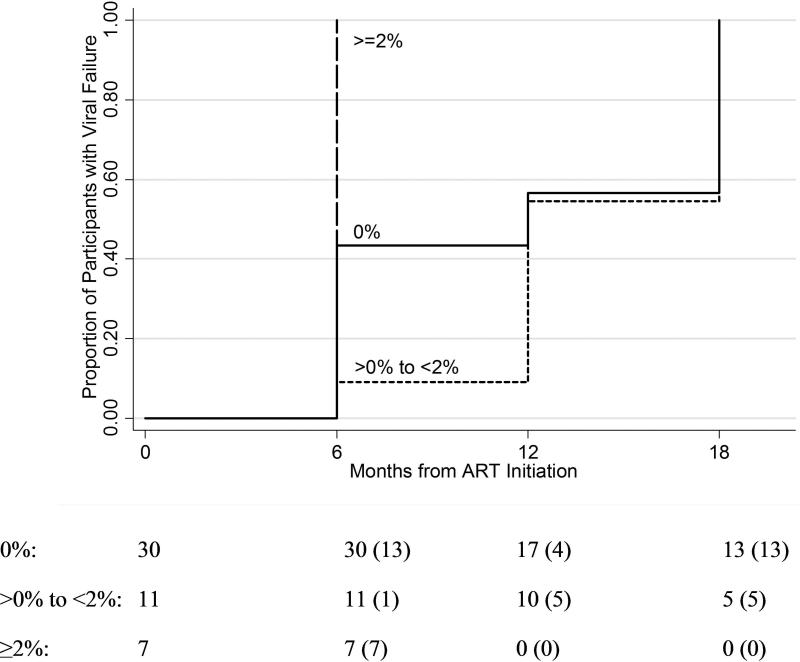
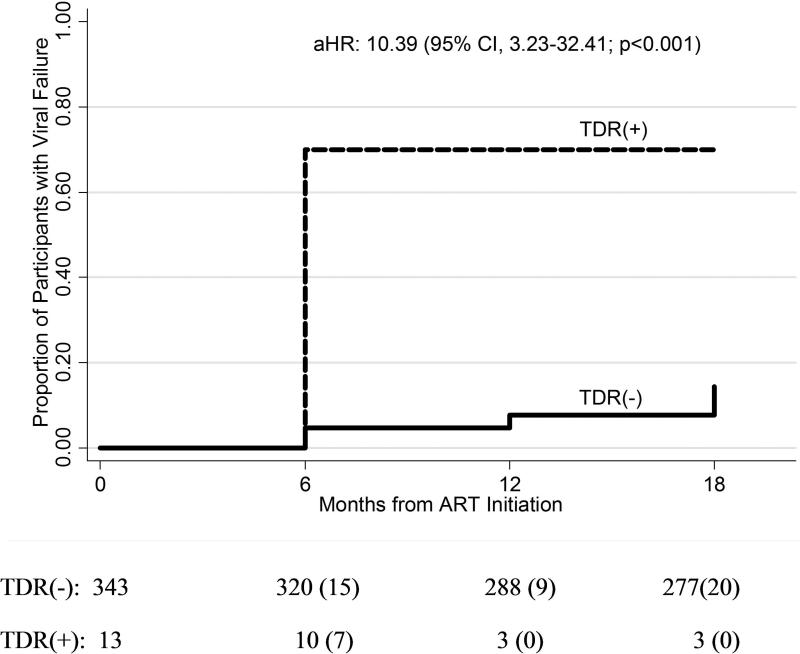
Among 386 participants, TDR was detected by OLA in 3.89% (95% confidence interval: 2.19 to 6.33) and was associated with a 10-fold higher rate of virologic failure (hazard ratio: 10.39; 95% confidence interval: 3.23 to 32.41; P < 0.001) compared with those without TDR. OLA detected 24 TDR mutations (K103N: n = 13; Y181C: n = 5; G190A: n = 3; M184V: n = 3) in 15 subjects (NNRTI: n = 15; 3TC: n = 3). Among 51 participants who developed virologic failure, consensus sequencing did not detect additional TDR mutations conferring high-level resistance, and pyrosequencing only detected additional mutations at frequencies <2%. Mutant frequencies <2% at ART initiation were significantly less likely to be found at the time of virologic failure compared with frequencies ≥2% (22% vs. 63%; P < 0.001).
Detection of TDR by a point mutation assay may prevent the use of suboptimal ART.
在非洲的一些地区,传播性耐药(TDR)正在增加。TDR的检测可能预测基于一线非核苷类逆转录酶抑制剂(NNRTI)的抗逆转录病毒疗法(ART)的病毒学失败。我们评估了一种相对廉价的寡核苷酸连接测定法(OLA)在ART启动时检测临床相关TDR的效用。
对2006年在一项随机依从性试验中开始基于NNRTI的固定剂量联合ART的未接受过ART的肯尼亚人的ART前血浆进行回顾性分析,通过OLA检测对NNRTI(K103N、Y181C和G190A)和拉米夫定(M184V)具有耐药性的突变。在18个月的随访期间,每隔6个月对ART后血浆进行病毒学失败(≥1000拷贝/mL)分析。对那些出现病毒学失败的患者的ART前血浆通过一致性测序和454焦磷酸测序评估耐药性。
在386名参与者中,OLA检测到TDR的比例为3.89%(95%置信区间:2.19至6.33),与未发生TDR的参与者相比,其病毒学失败率高10倍(风险比:10.39;95%置信区间:3.23至32.41;P<0.001)。OLA在15名受试者中检测到24个TDR突变(K103N:n = 13;Y181C:n = 5;G190A:n = 3;M184V:n = 3)(NNRTI:n = 15;3TC:n = 3)。在51名出现病毒学失败的参与者中,一致性测序未检测到其他赋予高水平耐药性的TDR突变,焦磷酸测序仅在频率<2%时检测到其他突变。与频率≥2%相比,ART启动时突变频率<2%在病毒学失败时被发现的可能性显著降低(22%对63%;P<0.001)。
通过点突变测定法检测TDR可能会避免使用次优的ART。