Division of Otolaryngology-Head and Neck Surgery, Department of Surgery, University of Alabama at Birmingham, Birmingham, AL.
Department of Surgery, University of Alabama at Birmingham, Birmingham, AL.
J Am Coll Surg. 2014 Oct;219(4):765-70. doi: 10.1016/j.jamcollsurg.2014.04.013. Epub 2014 May 29.
Previous intraoperative nerve monitoring (IONM) studies have demonstrated modest-to-no benefit and did not include a nationwide sample of hospitals representative of broad thyroidectomy practices. This national study was designed to compare vocal cord paralysis (VCP) rates between thyroidectomy with IONM and without monitoring (conventional).
We performed a retrospective analysis of 243,527 thyroidectomies during 2008 to 2011 using the Nationwide Inpatient Sample.
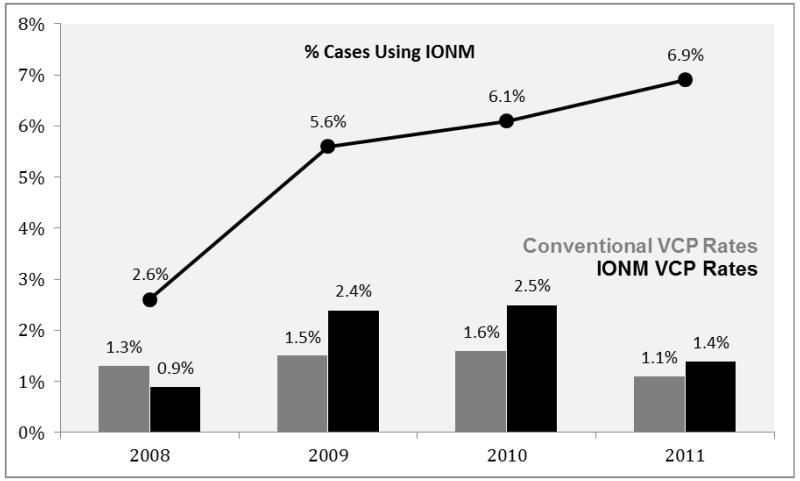
Use of IONM increased yearly throughout the study period (2.6% [2008], 5.6% [2009], 6.1% [2010], 6.9% [2011]) and during this time, VCP rates in the IONM group initially increased year-over-year (0.9% [2008], 2.4% [2009], 2.5% [2010], 1.4% [2011]). In unadjusted analyses, IONM was associated with significantly higher VCP rates (conventional 1.4% vs IONM 1.9%, p < 0.001). After propensity score matching, IONM remained associated with higher VCP rates in partial thyroidectomy and lower VCP rates for total thyroidectomy with neck dissection. Hospital-level analysis revealed that VCP rates were not explained by differential laryngoscopy rates, decreasing the likelihood of ascertainment bias. Additionally, for hospitals in which IONM was applied to more than 50% of thyroidectomies, lower VCP rates were observed (1.1%) compared with hospitals that applied IONM to less than 50% (1.6%, p = 0.016). Higher hospital volume correlated with lower VCP rates in both groups (<75, 75 to 299, >300 thyroidectomies/year: IONM, 2.1%, 1.7%, 1.7%; conventional, 1.5%, 1.3%, 1.0%, respectively).
According to this study, IONM has not been broadly adopted into practice. Overall, IONM was associated with a higher rate of VCP even after correction for numerous confounders. In particular, low institutional use of IONM and use in partial thyroidectomies are associated with higher rates of VCP. Further studies are warranted to support the broader application of IONM in patients where benefit can be reliably achieved.
先前的术中神经监测 (IONM) 研究表明,该监测方法的获益有限,且未纳入具有广泛甲状腺切除术实践代表性的全国范围内的医院样本。本项全国性研究旨在比较 IONM 辅助甲状腺切除术与无监测(常规)甲状腺切除术的声带麻痹 (VCP) 发生率。
我们使用 2008 年至 2011 年全国住院患者样本进行了回顾性分析。
在整个研究期间,IONM 的使用逐年增加(2008 年为 2.6%,2009 年为 5.6%,2010 年为 6.1%,2011 年为 6.9%),在此期间,IONM 组的 VCP 发生率逐年增加(2008 年为 0.9%,2009 年为 2.4%,2010 年为 2.5%,2011 年为 1.4%)。在未调整分析中,IONM 与更高的 VCP 发生率显著相关(常规组为 1.4%,IONM 组为 1.9%,p < 0.001)。经过倾向评分匹配后,IONM 仍与部分甲状腺切除术的更高 VCP 发生率相关,与全甲状腺切除术伴颈部清扫术的更低 VCP 发生率相关。医院层面的分析显示,VCP 发生率与不同的喉镜检查率无关,这降低了确定偏倚的可能性。此外,对于 IONM 应用于超过 50%甲状腺切除术的医院,VCP 发生率较低(1.1%),而 IONM 应用于不到 50%甲状腺切除术的医院则较高(1.6%,p = 0.016)。较高的医院手术量与两组的较低 VCP 发生率相关(<75、75-299、>300 例甲状腺切除术/年:IONM,2.1%、1.7%、1.7%;常规组,1.5%、1.3%、1.0%)。
根据本研究,IONM 尚未广泛应用于临床实践。尽管进行了多项混杂因素校正,IONM 总体上与更高的 VCP 发生率相关。特别是,机构中 IONM 的低使用率和在部分甲状腺切除术的应用与更高的 VCP 发生率相关。需要进一步的研究来支持 IONM 在能够可靠获益的患者中更广泛的应用。