Dobson R, Burgess M I, Valle J W, Pritchard D M, Vora J, Wong C, Chadwick C, Keevi B, Adaway J, Hofmann U, Poston G J, Cuthbertson D J
1] Neuroendocrine Tumour Group, University Hospital Aintree, Lower Lane, Liverpool L9 7AL, UK [2] Department of Obesity & Endocrinology, University of Liverpool, University Hospital Aintree, Lower Lane, Liverpool L9 7AL, UK.
1] Neuroendocrine Tumour Group, University Hospital Aintree, Lower Lane, Liverpool L9 7AL, UK [2] Department of Cardiology, University Hospital Aintree, Lower Lane, Liverpool L9 7AL, UK.
Br J Cancer. 2014 Oct 28;111(9):1703-9. doi: 10.1038/bjc.2014.468. Epub 2014 Sep 11.
Carcinoid heart disease is a complication of metastatic neuroendocrine tumours (NETs). We sought to identify factors associated with echocardiographic progression of carcinoid heart disease and death in patients with metastatic NETs.
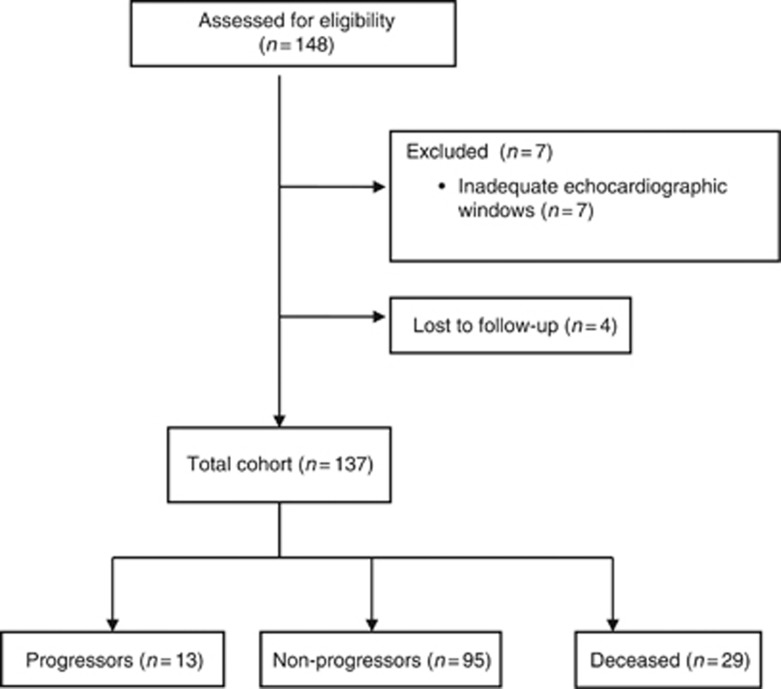
Patients with advanced non-pancreatic NETs and documented liver metastases and/or carcinoid syndrome underwent prospective serial clinical, biochemical, echocardiographic and radiological assessment. Patients were categorised as carcinoid heart disease progressors, non-progressors or deceased. Multinomial regression was used to assess the univariate association between variables and carcinoid heart disease progression.
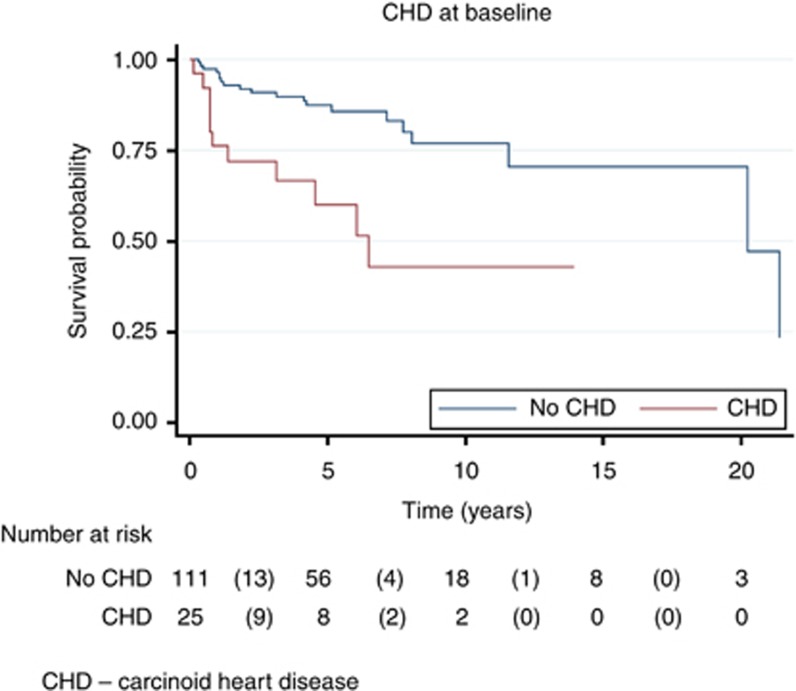
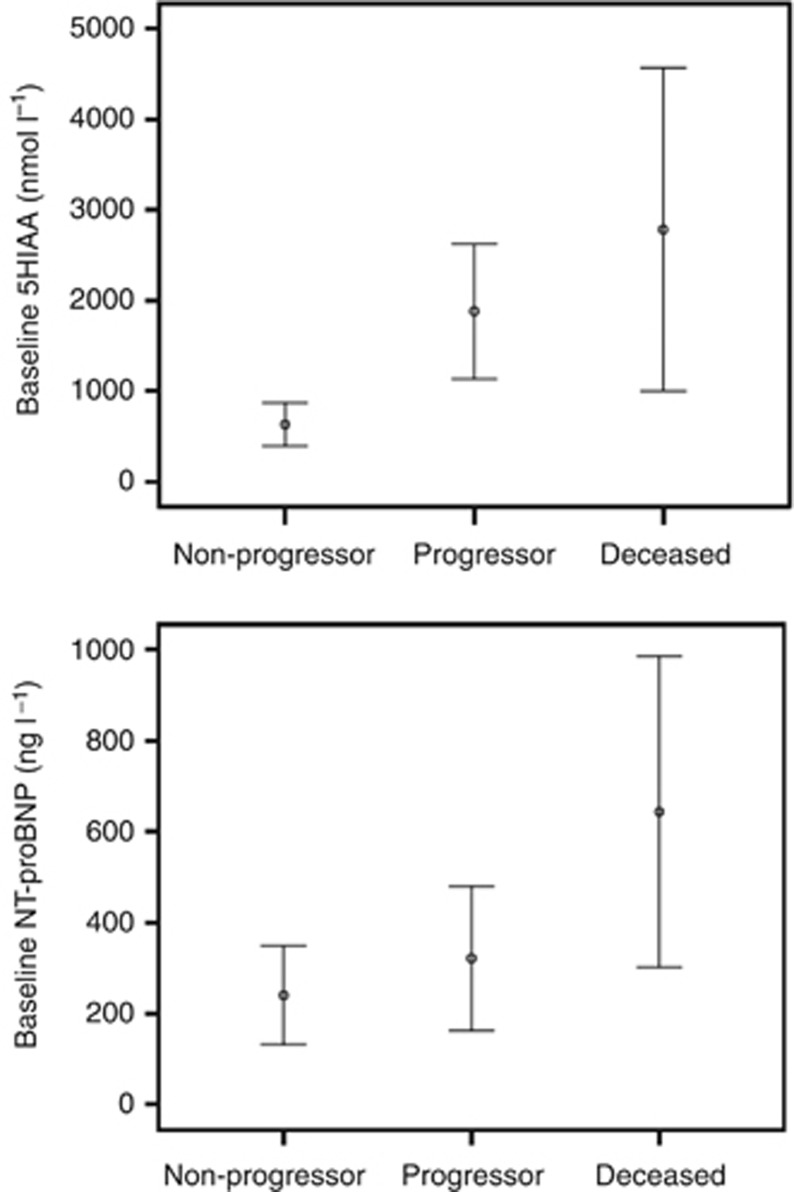
One hundred and thirty-seven patients were included. Thirteen patients (9%) were progressors, 95 (69%) non-progressors and 29 (21%) patients deceased. Baseline median levels of serum N-terminal pro-brain natriuretic peptide (NT-proBNP) and plasma 5-hydroxyindoleacetic acid (5-HIAA) were significantly higher in the progressors. Every 100 nmol l(-1) increase in 5-HIAA yielded a 5% greater odds of disease progression (OR 1.05, 95% CI: 1.01, 1.09; P=0.012) and a 7% greater odds of death (OR 1.07, 95% CI: 1.03, 1.10; P=0.001). A 100 ng l(-1) increase in NT-proBNP did not increase the risk of progression, but did increase the risk of death by 11%.
The biochemical burden of disease, in particular baseline plasma 5-HIAA concentration, is independently associated with carcinoid heart disease progression and death. Clinical and radiological factors are less useful prognostic indicators of carcinoid heart disease progression and/or death.
类癌性心脏病是转移性神经内分泌肿瘤(NETs)的一种并发症。我们试图确定与转移性NETs患者类癌性心脏病超声心动图进展及死亡相关的因素。
对患有晚期非胰腺NETs且有肝脏转移和/或类癌综合征记录的患者进行前瞻性系列临床、生化、超声心动图和放射学评估。患者被分类为类癌性心脏病进展者、非进展者或死亡者。采用多项回归分析评估变量与类癌性心脏病进展之间的单变量关联。
共纳入137例患者。13例(9%)为进展者,95例(69%)为非进展者,29例(21%)患者死亡。进展者的血清N末端脑钠肽前体(NT-proBNP)和血浆5-羟吲哚乙酸(5-HIAA)基线中位数水平显著更高。5-HIAA每升高100 nmol l⁻¹,疾病进展的几率增加5%(比值比1.05,95%置信区间:1.01,1.09;P = 0.012),死亡几率增加7%(比值比1.07,95%置信区间:1.03,1.10;P = 0.001)。NT-proBNP每升高100 ng l⁻¹,虽未增加进展风险,但死亡风险增加11%。
疾病的生化负担,尤其是基线血浆5-HIAA浓度,与类癌性心脏病进展及死亡独立相关。临床和放射学因素在类癌性心脏病进展和/或死亡的预后指标方面作用较小。