Vanderpool Rebecca R, Pinsky Michael R, Naeije Robert, Deible Christopher, Kosaraju Vijaya, Bunner Cheryl, Mathier Michael A, Lacomis Joan, Champion Hunter C, Simon Marc A
Vascular Medicine Institute, University of Pittsburgh, Pittsburgh, Pennsylvania, USA.
Heart & Vascular Institute, University of Pittsburgh, Pittsburgh, Pennsylvania, USA Department of Bioengineering, University of Pittsburgh, Pittsburgh, Pennsylvania, USA Department of Critical Care Medicine, University of Pittsburgh, Pittsburgh, Pennsylvania, USA.
Heart. 2015 Jan;101(1):37-43. doi: 10.1136/heartjnl-2014-306142. Epub 2014 Sep 11.
Prognosis in pulmonary hypertension (PH) is largely determined by RV function. However, uncertainty remains about what metrics of RV function might be most clinically relevant. The purpose of this study was to assess the clinical relevance of metrics of RV functional adaptation to increased afterload.
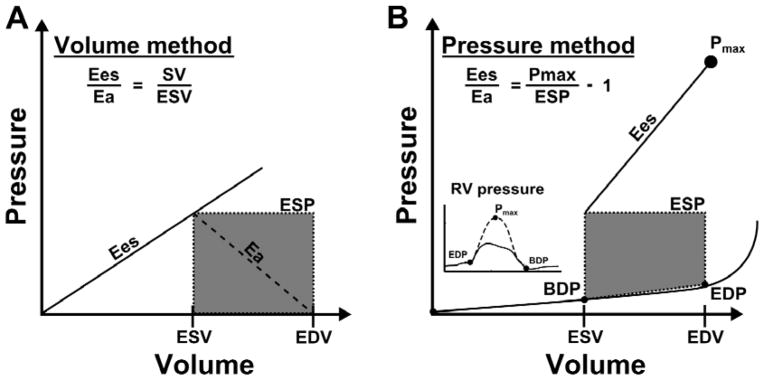
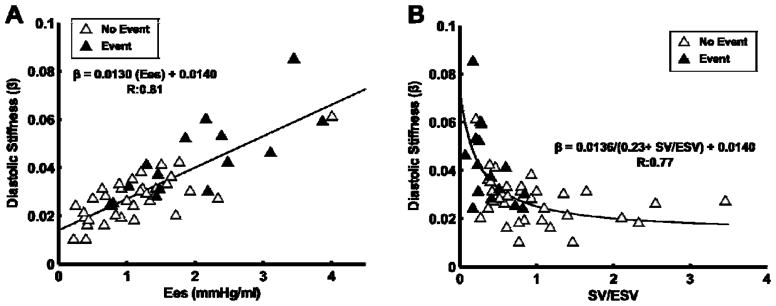
Patients referred for PH underwent right heart catheterisation and RV volumetric assessment within 48 h. A RV maximum pressure (Pmax) was calculated from the RV pressure curve. The adequacy of RV systolic functional adaptation to increased afterload was estimated either by a stroke volume (SV)/end-systolic volume (ESV) ratio, a Pmax/mean pulmonary artery pressure (mPAP) ratio, or by EF (RVEF). Diastolic function of the RV was estimated by a diastolic elastance coefficient β. Survival analysis was via Cox proportional HR, and Kaplan-Meier with the primary outcome of time to death or lung transplant.
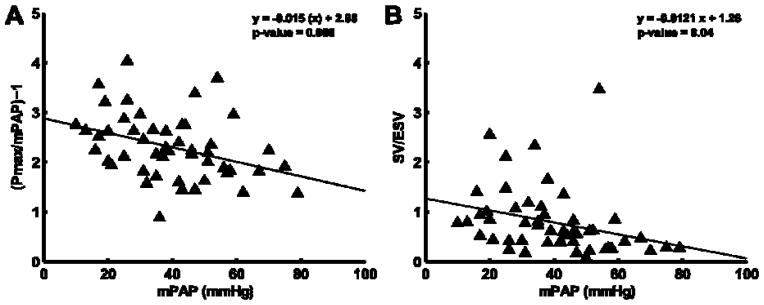
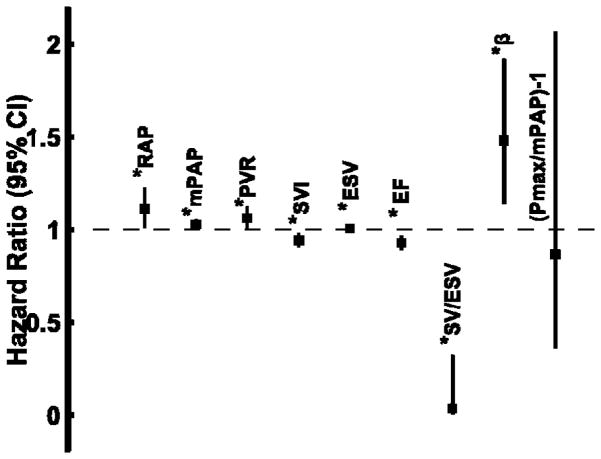
Patients (n=50; age 58±13 yrs) covered a range of mPAP (13-79 mm Hg) with an average RVEF of 39±17% and ESV of 143±89 mL. Average estimates of the ratio of end-systolic ventricular to arterial elastance were 0.79±0.67 (SV/ESV) and 2.3±0.65 (Pmax/mPAP-1). Transplantation-free survival was predicted by right atrial pressure, mPAP, pulmonary vascular resistance, β, SV, ESV, SV/ESV and RVEF, but after controlling for right atrial pressure, mPAP, and SV, SV/ESV was the only independent predictor.
The adequacy of RV functional adaptation to afterload predicts survival in patients referred for PH. Whether this can simply be evaluated using RV volumetric imaging will require additional confirmation.
肺动脉高压(PH)的预后很大程度上由右心室(RV)功能决定。然而,关于RV功能的哪些指标可能在临床上最具相关性仍存在不确定性。本研究的目的是评估RV功能适应后负荷增加的指标的临床相关性。
因PH就诊的患者在48小时内接受了右心导管检查和RV容积评估。从RV压力曲线计算出RV最大压力(Pmax)。通过每搏输出量(SV)/收缩末期容积(ESV)比值、Pmax/平均肺动脉压(mPAP)比值或射血分数(RVEF)来评估RV收缩功能适应后负荷增加的充分性。通过舒张弹性系数β评估RV的舒张功能。生存分析采用Cox比例风险比,以及以死亡或肺移植时间为主要结局的Kaplan-Meier法。
患者(n = 50;年龄58±13岁)的mPAP范围为13 - 79 mmHg,平均RVEF为39±17%,ESV为143±89 mL。收缩末期心室与动脉弹性比值的平均估计值分别为0.79±0.67(SV/ESV)和2.3±0.65(Pmax/mPAP - 1)。无移植生存可由右心房压力、mPAP、肺血管阻力、β、SV、ESV、SV/ESV和RVEF预测,但在控制右心房压力、mPAP和SV后,SV/ESV是唯一的独立预测因素。
RV功能适应后负荷的充分性可预测因PH就诊患者的生存情况。是否可以简单地通过RV容积成像进行评估还需要进一步证实。