Kim In Kyong, Lee Joo Yong, Kwon Jong Kyou, Park Jae Joon, Cho Kang Su, Ham Won Sik, Hong Sung Joon, Yang Seung Choul, Choi Young Deuk
Department of Urology, Severance Hospital, Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea.
Department of Urology, Gangnam Severance Hospital, Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea.
Korean J Urol. 2014 Sep;55(9):574-80. doi: 10.4111/kju.2014.55.9.574. Epub 2014 Sep 5.
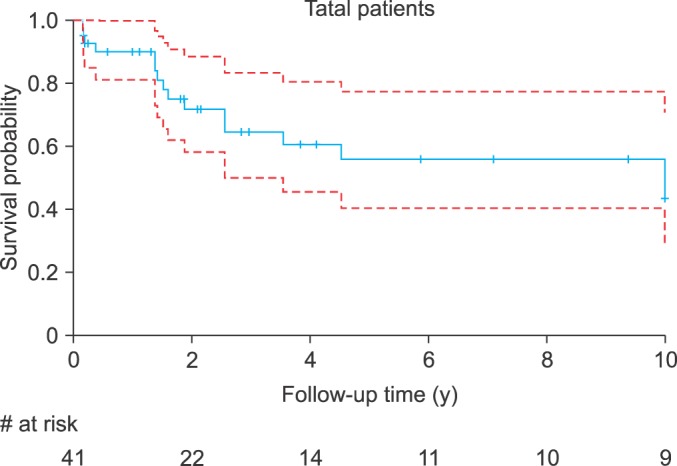
This study was conducted to evaluate prognostic factors and cancer-specific survival (CSS) in a cohort of 41 patients with urachal carcinoma by use of a Bayesian model-averaging approach.
Our cohort included 41 patients with urachal carcinoma who underwent extended partial cystectomy, total cystectomy, transurethral resection, chemotherapy, or radiotherapy at a single institute. All patients were classified by both the Sheldon and the Mayo staging systems according to histopathologic reports and preoperative radiologic findings. Kaplan-Meier survival curves and Cox proportional-hazards regression models were carried out to investigate prognostic factors, and a Bayesian model-averaging approach was performed to confirm the significance of each variable by using posterior probabilities.
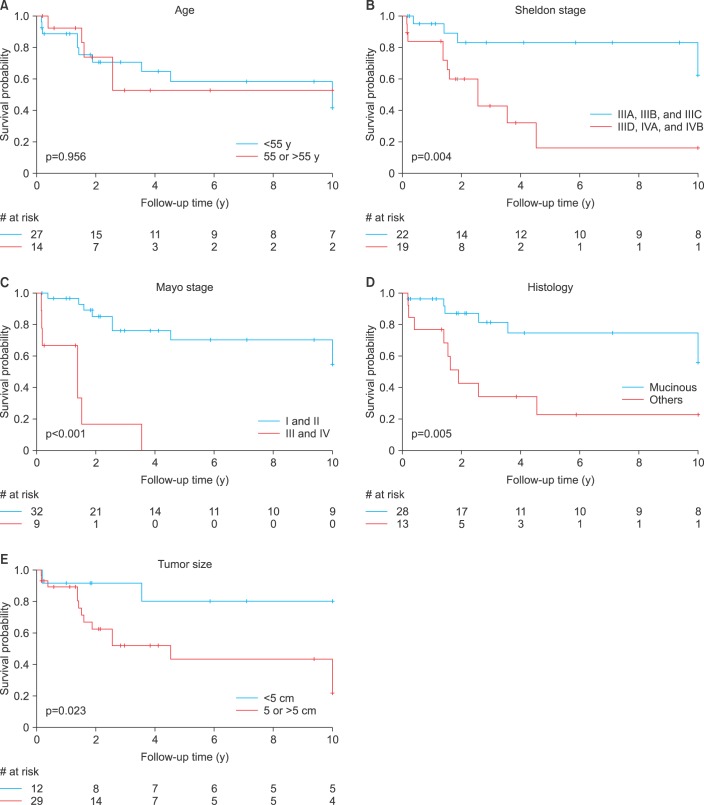
The mean age of the patients was 49.88 ± 13.80 years and the male-to-female ratio was 24:17. The median follow-up was 5.42 years (interquartile range, 2.8-8.4 years). Five- and 10-year CSS rates were 55.9% and 43.4%, respectively. Lower Sheldon (p=0.004) and Mayo (p<0.001) stage, mucinous adenocarcinoma (p=0.005), and larger tumor size (p=0.023) were significant predictors of high survival probability on the basis of a log-rank test. By use of the Bayesian model-averaging approach, higher Mayo stage and larger tumor size were significant predictors of cancer-specific mortality in urachal carcinoma.
The Mayo staging system might be more effective than the Sheldon staging system. In addition, the multivariate analyses suggested that tumor size may be a prognostic factor for urachal carcinoma.
本研究旨在通过贝叶斯模型平均法评估41例脐尿管癌患者的预后因素及癌症特异性生存率(CSS)。
我们的队列包括41例脐尿管癌患者,这些患者在单一机构接受了扩大部分膀胱切除术、全膀胱切除术、经尿道切除术、化疗或放疗。根据组织病理学报告和术前影像学检查结果,所有患者均按照谢尔登(Sheldon)分期系统和梅奥(Mayo)分期系统进行分类。采用Kaplan-Meier生存曲线和Cox比例风险回归模型研究预后因素,并通过贝叶斯模型平均法利用后验概率确定每个变量的显著性。
患者的平均年龄为49.88±13.80岁,男女比例为24:17。中位随访时间为5.42年(四分位间距,2.8 - 8.4年)。5年和10年CSS率分别为55.9%和43.4%。基于对数秩检验,较低的谢尔登分期(p = 0.004)和梅奥分期(p < 0.001)、黏液腺癌(p = 0.005)以及较大的肿瘤大小(p = 0.023)是高生存概率的显著预测因素。通过贝叶斯模型平均法,较高的梅奥分期和较大的肿瘤大小是脐尿管癌癌症特异性死亡的显著预测因素。
梅奥分期系统可能比谢尔登分期系统更有效。此外,多变量分析表明肿瘤大小可能是脐尿管癌的一个预后因素。