Skarphedinsson Gudmundur, Weidle Bernhard, Thomsen Per Hove, Dahl Kitty, Torp Nor Christian, Nissen Judith B, Melin Karin Holmgren, Hybel Katja, Valderhaug Robert, Wentzel-Larsen Tore, Compton Scott N, Ivarsson Tord
Center for Child and Adolescent Mental Health, Eastern and Southern Norway, Gullhaugveien 1-3, 0484, Oslo, Norway,
Eur Child Adolesc Psychiatry. 2015 May;24(5):591-602. doi: 10.1007/s00787-014-0613-0. Epub 2014 Sep 20.
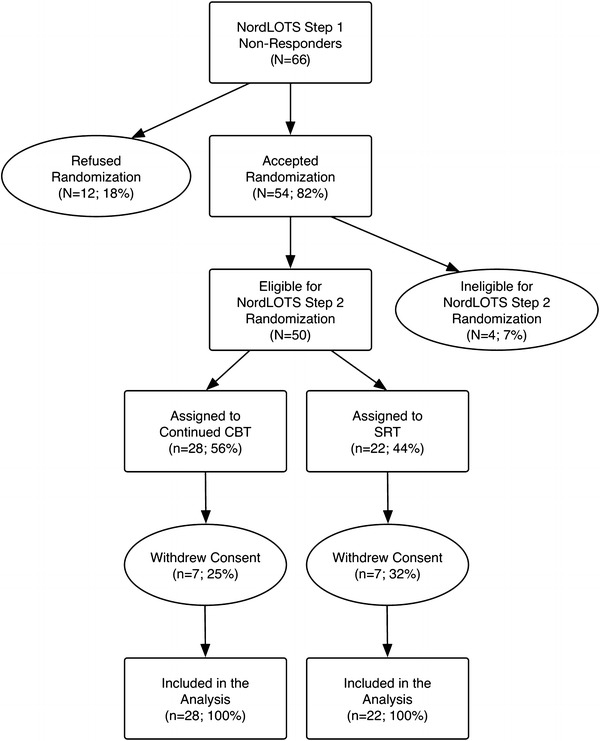
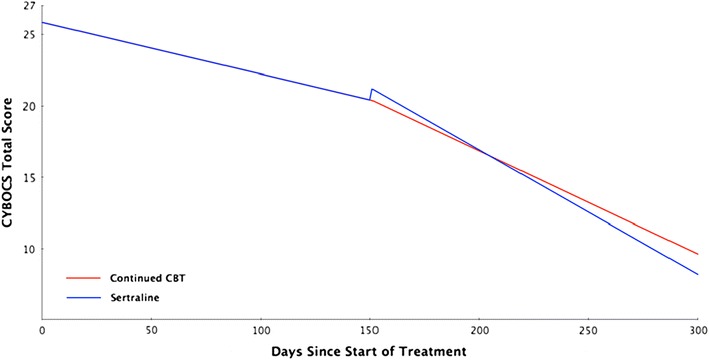
Expert guidelines recommend cognitive-behavior therapy (CBT) as a first-line treatment in pediatric obsessive-compulsive disorder (OCD) and the addition of selective serotonin reuptake inhibitors when CBT is not effective. However, the recommendations for CBT non-responders are not supported by empirical data. Our objective was to investigate the effectiveness of sertraline (SRT) versus continued CBT in children and adolescents that did not respond to an initial course of CBT. Randomized controlled trial conducted in five sites in Denmark, Sweden and Norway, 54 children and adolescents, age 7-17 years, with DSM-IV primary OCD were randomized to SRT or continued CBT for 16 weeks. These participants had been classified as non-responders to CBT following 14 weekly sessions. Primary outcomes were the CY-BOCS total score and clinical response (CY-BOCS <16). The study was a part of the Nordic Long-Term OCD Treatment Study (NordLOTS). Intent-to-treat sample included 50 participants, mean age 14.0 (SD = 2.7) and 48 (n = 24) males. Twenty-one of 28 participants (75%) completed continued CBT and 15 of 22 participants (69.2%) completed SRT. Planned pairwise comparison of the CY-BOCS total score did not reveal a significant difference between the treatments (p = .351), the response rate was 50.0% in the CBT group and 45.4% in the SRT group. The multivariate χ (2) test suggested that there were no statistically significant differences between groups (p = .727). Within-group effect sizes were large and significant across both treatments. These large within-group effect sizes suggest that continued treatment for CBT non-responders is beneficial. However, there was no significant between-group differences in SRT or continued CBT at post-treatment.
专家指南推荐认知行为疗法(CBT)作为儿童强迫症(OCD)的一线治疗方法,当CBT无效时加用选择性5-羟色胺再摄取抑制剂。然而,针对CBT无反应者的推荐缺乏实证数据支持。我们的目的是调查舍曲林(SRT)与继续进行CBT相比,对未对初始疗程CBT产生反应的儿童和青少年的有效性。在丹麦、瑞典和挪威的五个地点进行了随机对照试验,54名年龄在7至17岁、患有DSM-IV原发性OCD的儿童和青少年被随机分为SRT组或继续进行CBT组,为期16周。这些参与者在接受14次每周疗程后被归类为CBT无反应者。主要结局指标为儿童耶鲁-布朗强迫症量表(CY-BOCS)总分及临床反应(CY-BOCS<16)。该研究是北欧长期强迫症治疗研究(NordLOTS)的一部分。意向性治疗样本包括50名参与者,平均年龄14.0(标准差=2.7),男性48名(n=24)。28名参与者中有21名(75%)完成了继续CBT,22名参与者中有15名(69.2%)完成了SRT。CY-BOCS总分的计划成对比较未显示治疗组间存在显著差异(p=0.351),CBT组的反应率为50.0%,SRT组为45.4%。多变量χ²检验表明组间无统计学显著差异(p=0.727)。两组治疗的组内效应量均较大且显著。这些较大的组内效应量表明,对CBT无反应者继续治疗是有益的。然而,治疗后SRT组与继续CBT组之间无显著组间差异。