Matzaroglou Charalampos, Georgiou Christos S, Panagopoulos Andreas, Assimakopoulos Kostantinos, Wilke Hans J, Habermann Bjoern, Panos George, Kafchitsas Konstantinos
Department of Orthopaedic Surgery, University of Patras, Greece.
Department of Psychiatry, University of Patras, Greece.
Open Orthop J. 2014 Sep 15;8:288-97. doi: 10.2174/1874325001408010288. eCollection 2014.
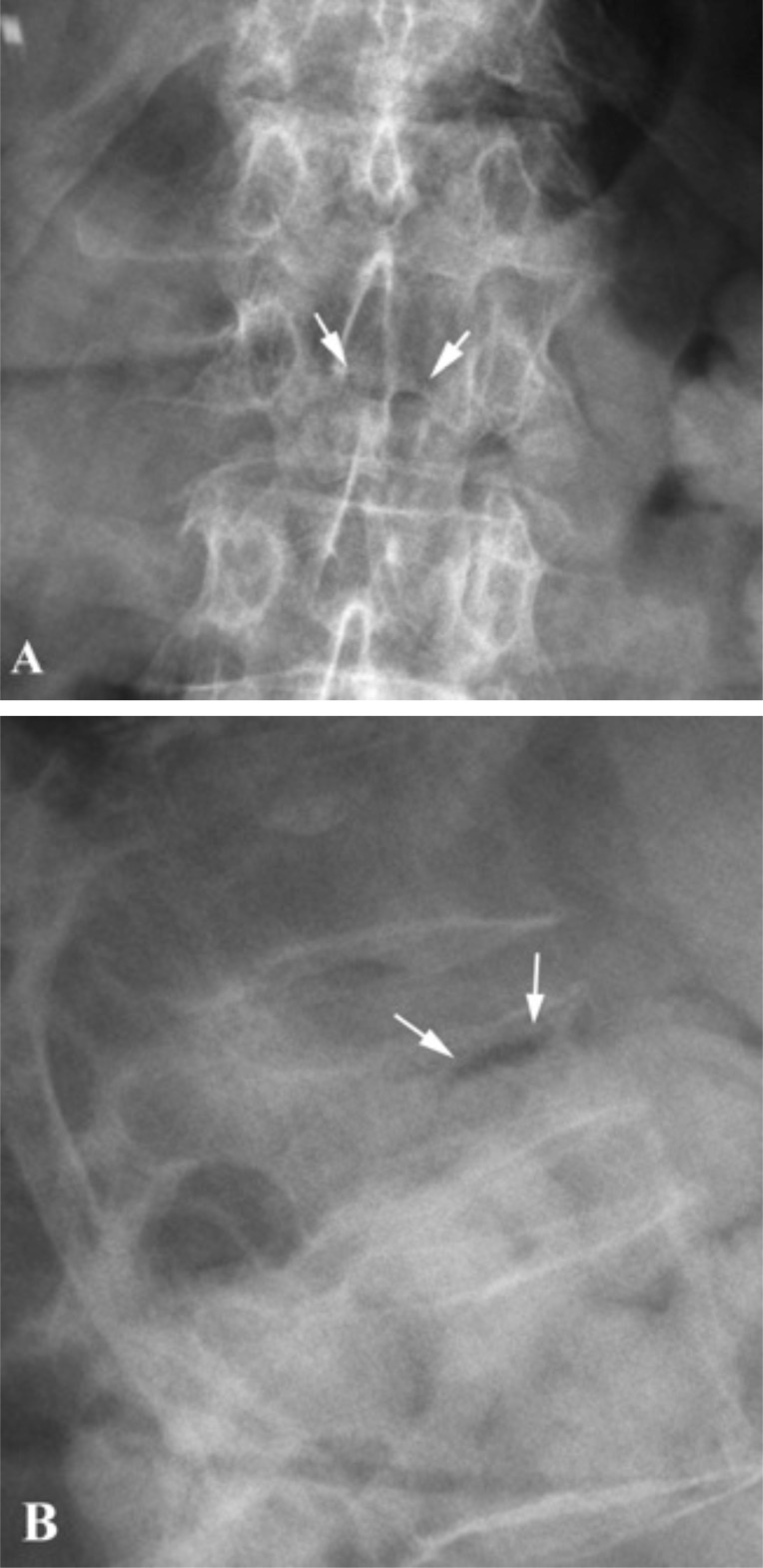
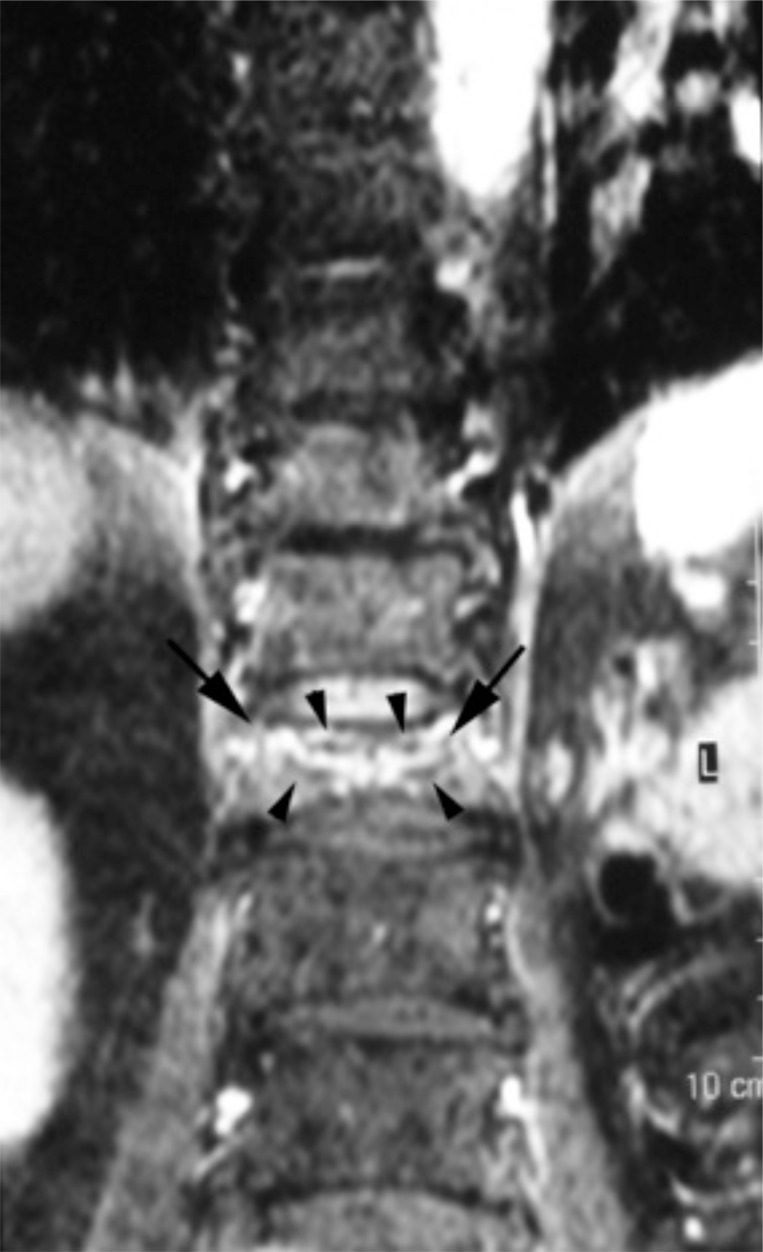
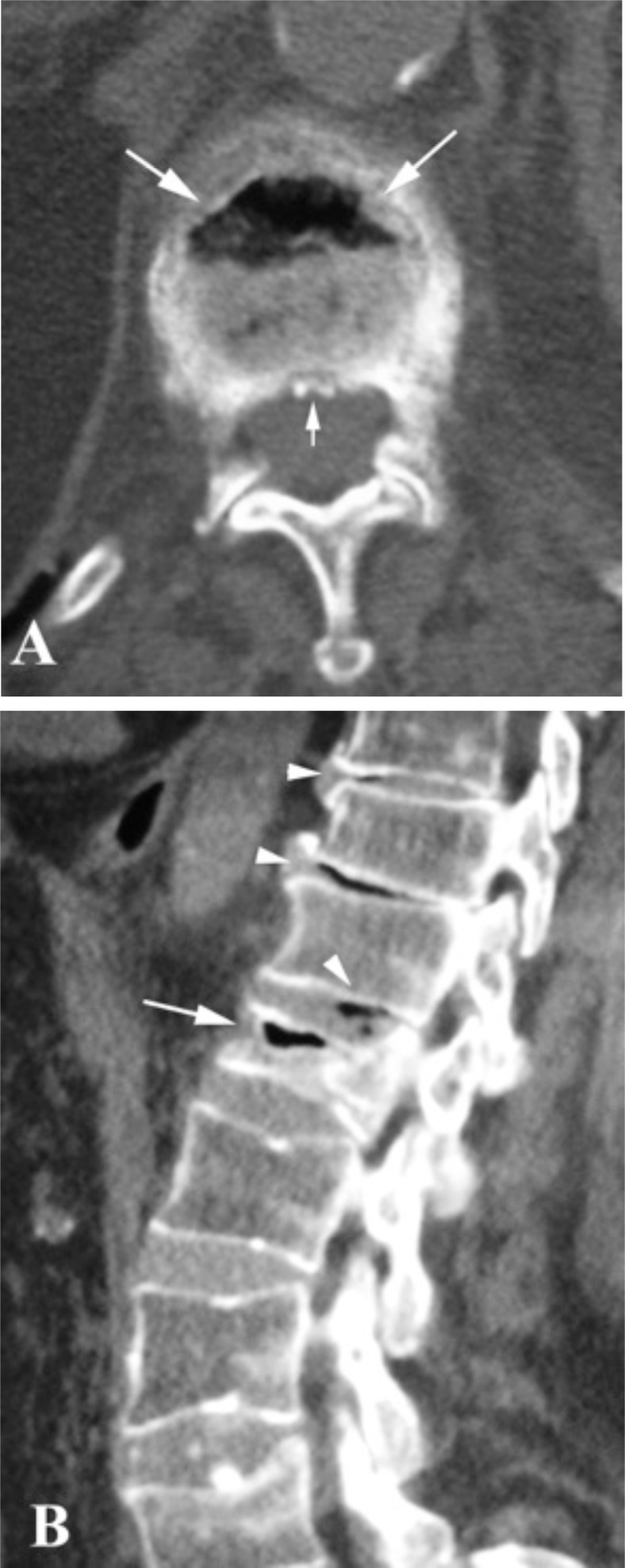
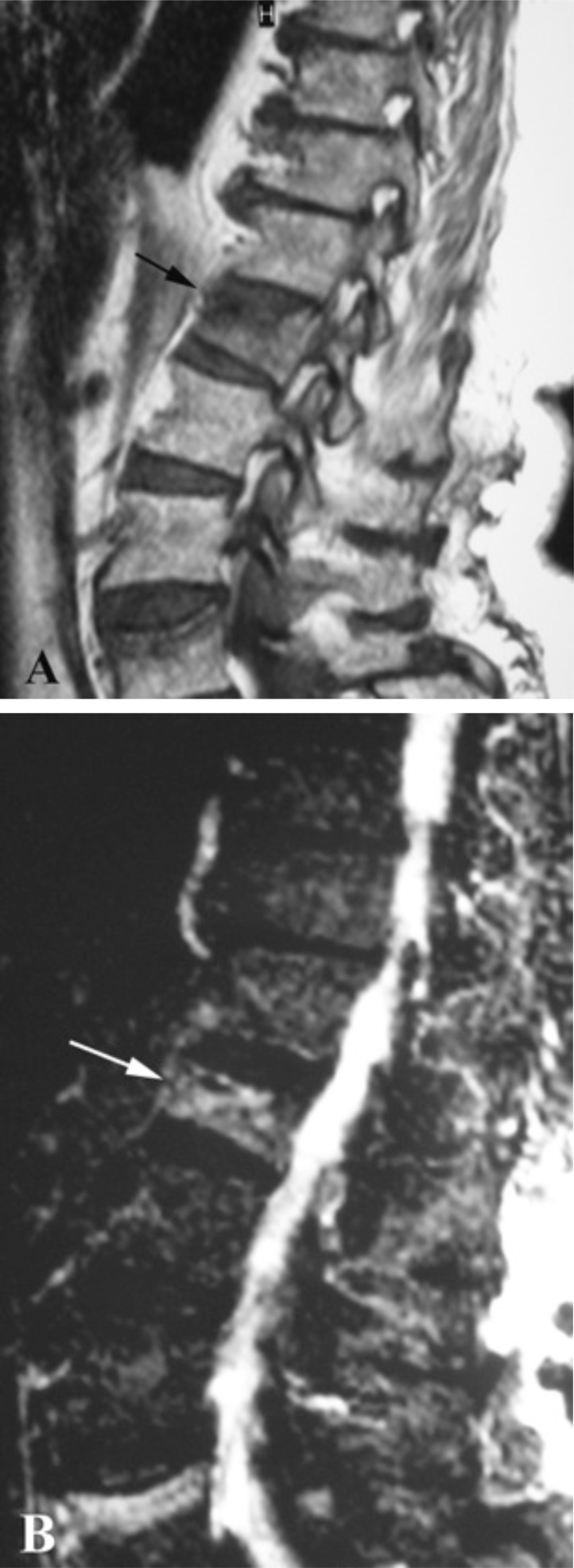
The three major causes of vertebral body collapse include infection, malignant neoplasia, and trauma and it may be difficult to distinguish between them, particularly in the presence of severe osteoporosis. In 1891, however, Dr Hermann Kümmell, further added another possibility of vertebral body crush; the delayed posttraumatic collapse. As originally described, this rare clinical entity includes patients, who after a trivial trauma and an asymptomatic clinical course they develop a progressive vertebral body collapse and a painful kyphosis. Although more than a century has passed from its initial description, only few cases have been reported in the literature, whereas the main pathologic eliciting event is still under investigation. As a consequence, great controversy exists regarding the discrete features of the clinical course, its radiographic appearance and the histopathological findings. To explain the time lag between the initial trauma and the occurrence of the vertebral collapse, the hypothesis of ischemic necrosis was advanced. Equation of Kümmell's disease with vertebral osteonecrosis, however, has wrongly led many authors to report cases of Kümmell's disease, even in the absence of history of spinal trauma. On the other hand, high coincidence of vertebral osteonecrosis and the pathognomonic radiographic finding of intravertebral vacuum cleft, has further added to the confusion. In this review we present an overview of the literature on Kümmell's disease, focusing on the different proposed eliciting mechanisms. We also highlight controversial subjects on clinical course, diagnosis and treatment of this entity, in an attempt to further clarify patients' inclusion criteria.
椎体塌陷的三大主要原因包括感染、恶性肿瘤和创伤,区分它们可能存在困难,尤其是在严重骨质疏松的情况下。然而,1891年,赫尔曼·屈梅尔博士进一步提出了椎体压缩的另一种可能性,即创伤后延迟性塌陷。最初描述时,这种罕见的临床病症包括一些患者,他们在经历轻微创伤且临床过程无症状后,会出现椎体渐进性塌陷和疼痛性驼背。尽管自最初描述以来已过去一个多世纪,但文献中报道的病例很少,而主要的病理引发事件仍在研究中。因此,关于临床病程的离散特征、其影像学表现和组织病理学发现存在很大争议。为了解释初始创伤与椎体塌陷发生之间的时间间隔,有人提出了缺血性坏死的假说。然而,将屈梅尔病等同于椎体骨坏死,错误地导致许多作者报告屈梅尔病病例,甚至在没有脊柱创伤史的情况下也是如此。另一方面,椎体骨坏死与椎体内真空裂隙的特征性影像学表现高度吻合,这进一步加剧了混乱。在本综述中,我们概述了关于屈梅尔病的文献,重点关注不同的提出的引发机制。我们还强调了关于该病症临床病程、诊断和治疗的有争议的主题,试图进一步明确患者的纳入标准。