Goh Louise Gek Huang, Welborn Timothy Alexander, Dhaliwal Satvinder Singh
School of Public Health, Curtin Health Innovation Research Institute (CHIRI), Curtin University, Perth, Australia.
BMC Womens Health. 2014 Sep 26;14:118. doi: 10.1186/1472-6874-14-118.
We conducted an independent external validation of three cardiovascular risk score models (Framingham risk score model and SCORE risk charts developed for low-risk regions and high-risk regions in Europe) on a prospective cohort of 4487 Australian women with no previous history of heart disease, diabetes or stroke. External validation is an important step to evaluate the performance of risk score models using discrimination and calibration measures to ensure their applicability beyond the settings in which they were developed.
Ten year mortality follow-up of 4487 Australian adult women from the National Heart Foundation third Risk Factor Prevalence Study with no baseline history of heart disease, diabetes or stroke. The 10-year risk of cardiovascular mortality was calculated using the Framingham and SCORE models and the predictive accuracy of the three risk score models were assessed using both discrimination and calibration.
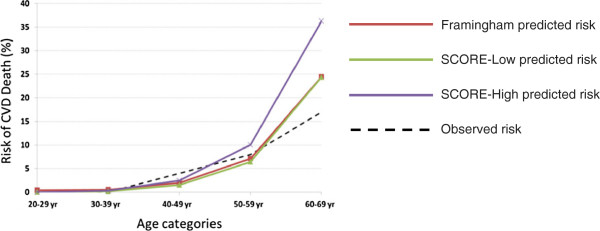
The discriminative ability of the Framingham and SCORE models were good (area under the curve > 0.85). Although all models overestimated the number of cardiovascular deaths by greater than 15%, the Hosmer-Lemeshow test indicated that the Framingham and SCORE-Low models were calibrated and hence suitable for predicting the 10-year cardiovascular mortality risk in this Australian population. An assessment of the treatment thresholds for each of the three models in identifying participants recommended for treatment were found to be inadequate, with low sensitivity and high specificity resulting from the high recommended thresholds. Lower treatment thresholds of 8.7% for the Framingham model, 0.8% for the SCORE-Low model and 1.3% for the SCORE-High model were identified for each model using the Youden index, at greater than 78% sensitivity and 80% specificity.
Framingham risk score model and SCORE risk chart for low-risk regions are recommended for use in the Australian women population for predicting the 10-year cardiovascular mortality risk. These models demonstrate good discrimination and calibration performance. Lower treatment thresholds are proposed for better identification of individuals for treatment.
我们对4487名无心脏病、糖尿病或中风病史的澳大利亚女性前瞻性队列进行了三种心血管风险评分模型(弗雷明汉风险评分模型以及为欧洲低风险地区和高风险地区开发的SCORE风险图表)的独立外部验证。外部验证是使用区分度和校准指标评估风险评分模型性能的重要步骤,以确保其在开发环境之外的适用性。
对来自澳大利亚国家心脏基金会第三次风险因素患病率研究的4487名成年女性进行了十年死亡率随访,这些女性无心脏病、糖尿病或中风的基线病史。使用弗雷明汉模型和SCORE模型计算心血管疾病死亡率的10年风险,并使用区分度和校准评估三种风险评分模型的预测准确性。
弗雷明汉模型和SCORE模型的区分能力良好(曲线下面积>0.85)。尽管所有模型对心血管死亡人数的高估均超过15%,但霍斯默-莱梅肖检验表明,弗雷明汉模型和SCORE-低风险模型经过校准,因此适用于预测该澳大利亚人群的10年心血管疾病死亡风险。发现三种模型在识别推荐治疗参与者时的治疗阈值评估不足,由于推荐阈值较高,导致敏感性低而特异性高。使用约登指数为每个模型确定的较低治疗阈值分别为:弗雷明汉模型8.7%、SCORE-低风险模型0.8%和SCORE-高风险模型1.3%,敏感性大于78%,特异性大于80%。
推荐使用弗雷明汉风险评分模型和低风险地区的SCORE风险图表来预测澳大利亚女性人群的10年心血管疾病死亡风险。这些模型具有良好的区分度和校准性能。为更好地识别需要治疗的个体,提出了更低的治疗阈值。