1 School of Population and Global Health, University of Melbourne, Australia.
2 Centre for Chronic Disease Prevention, James Cook University, Australia.
Eur J Prev Cardiol. 2017 Oct;24(15):1660-1669. doi: 10.1177/2047487317722913. Epub 2017 Jul 27.
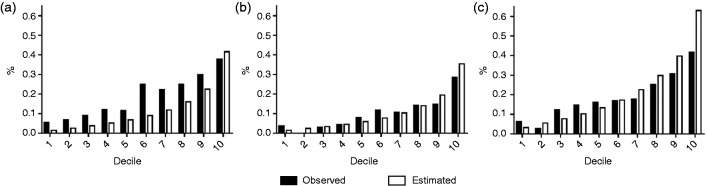
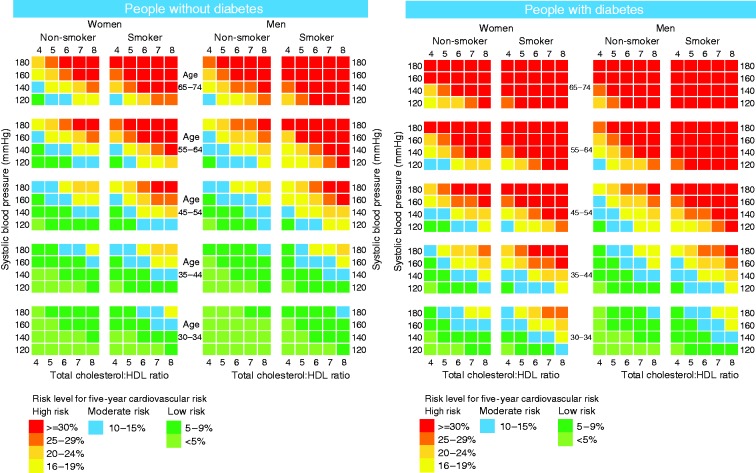
Background In Australia, clinical guidelines for primary prevention of cardiovascular disease recommend the use of the Framingham model to help identify those at high risk of developing the disease. However, this model has not been validated for the Indigenous population. Design Cohort study. Methods Framingham models were applied to the Well Person's Health Check (WPHC) cohort (followed 1998-2014), which included 1448 Aboriginal and Torres Strait Islanders from remote Indigenous communities in Far North Queensland. Cardiovascular disease risk predicted by the original and recalibrated Framingham models were compared with the observed risk in the WPHC cohort. Results The observed five- and 10-year cardiovascular disease probability of the WPHC cohort was 10.0% (95% confidence interval (CI): 8.5-11.7) and 18.7% (95% CI: 16.7-21.0), respectively. The Framingham models significantly underestimated the cardiovascular disease risk for this cohort by around one-third, with a five-year cardiovascular disease risk estimate of 6.8% (95% CI: 6.4-7.2) and 10-year risk estimates of 12.0% (95% CI: 11.4-12.6) and 14.2% (95% CI: 13.5-14.8). The original Framingham models showed good discrimination ability (C-statistic of 0.67) but a significant lack of calibration (χ between 82.56 and 134.67). After recalibration the 2008 Framingham model corrected the underestimation and improved the calibration for five-year risk prediction (χ of 18.48). Conclusions The original Framingham models significantly underestimate the absolute cardiovascular disease risk for this Australian Indigenous population. The recalibrated 2008 Framingham model shows good performance on predicting five-year cardiovascular disease risk in this population and was used to calculate the first risk chart based on empirical validation using long-term follow-up data from a remote Australian Indigenous population.
在澳大利亚,心血管疾病一级预防的临床指南建议使用 Framingham 模型来帮助识别那些有患病风险的人。然而,该模型尚未针对原住民进行验证。
队列研究。
Framingham 模型应用于 1998-2014 年期间参加健康体检的人群(简称 WPHC 队列),该队列包含来自昆士兰州北部偏远原住民社区的 1448 名原住民和托雷斯海峡岛民。比较原始 Framingham 模型和重新校准的 Framingham 模型预测的心血管疾病风险与 WPHC 队列中的观察风险。
WPHC 队列的五年和十年心血管疾病发生率分别为 10.0%(95%置信区间:8.5-11.7)和 18.7%(95%置信区间:16.7-21.0)。Framingham 模型显著低估了该队列的心血管疾病风险,五年心血管疾病风险估计值为 6.8%(95%置信区间:6.4-7.2),十年风险估计值为 12.0%(95%置信区间:11.4-12.6)和 14.2%(95%置信区间:13.5-14.8)。原始 Framingham 模型具有良好的区分能力(C 统计量为 0.67),但校准效果不佳(χ值为 82.56-134.67)。重新校准后,2008 年 Framingham 模型纠正了低估,改善了五年风险预测的校准(χ值为 18.48)。
原始 Framingham 模型显著低估了澳大利亚原住民人群的心血管疾病绝对风险。重新校准的 2008 年 Framingham 模型在预测该人群五年心血管疾病风险方面表现良好,并使用来自偏远澳大利亚原住民人群的长期随访数据进行了实证验证,在此基础上生成了第一张风险图表。