Lang Sean M, Syed Mansoor A, Dziura James, Rocco Edward, Kirshbom Paul, Bhandari Vineet, Giuliano John S
Department of Pediatrics, The Heart Institute, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio.
Department of Pediatrics, Division of Perinatal Medicine, Yale University School of Medicine, New Haven, Connecticut.
Ann Thorac Surg. 2014 Nov;98(5):1699-704. doi: 10.1016/j.athoracsur.2014.06.053. Epub 2014 Sep 23.
Cardiopulmonary bypass subjects patients' blood to hemodilution and nonphysiologic conditions, resulting in a systemic inflammatory response. Modified ultrafiltration (MUF) counteracts hemodilution and has also been postulated to improve outcomes by proinflammatory cytokine removal. The objective of this study was to investigate whether the benefits of MUF include the removal of proinflammatory mediators, such as angiopoietin-2 (angpt-2). We hypothesize that some of the clinical benefits of MUF are related to the preferential removal of angpt-2.
We performed a prospective cohort study in children 18 years old or younger undergoing cardiopulmonary bypass. Serum samples were obtained from each patient preoperatively, after cardiopulmonary bypass, and on intensive care unit admission. A fluid sample from the MUF effluent was also analyzed. Angpt-1, angpt-2, interleukin-8, and interleukin-10 levels were determined by enzyme-linked immunosorbent assay.
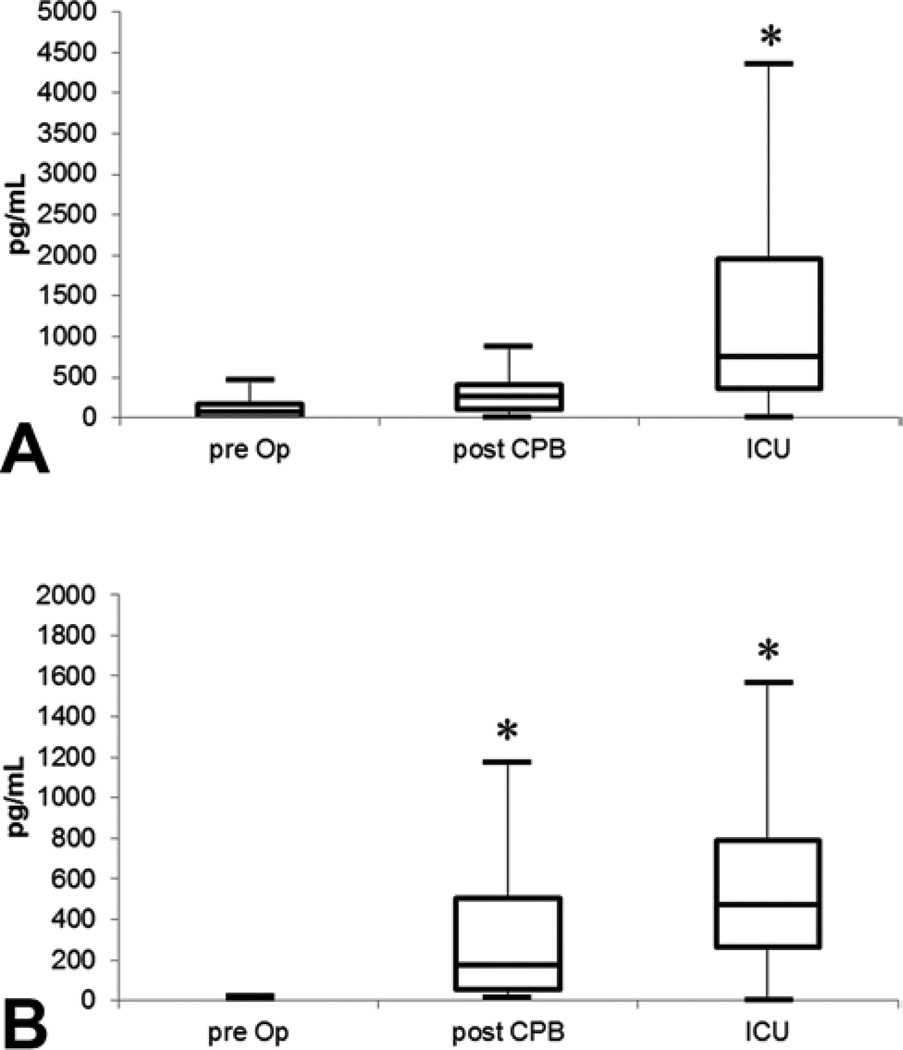
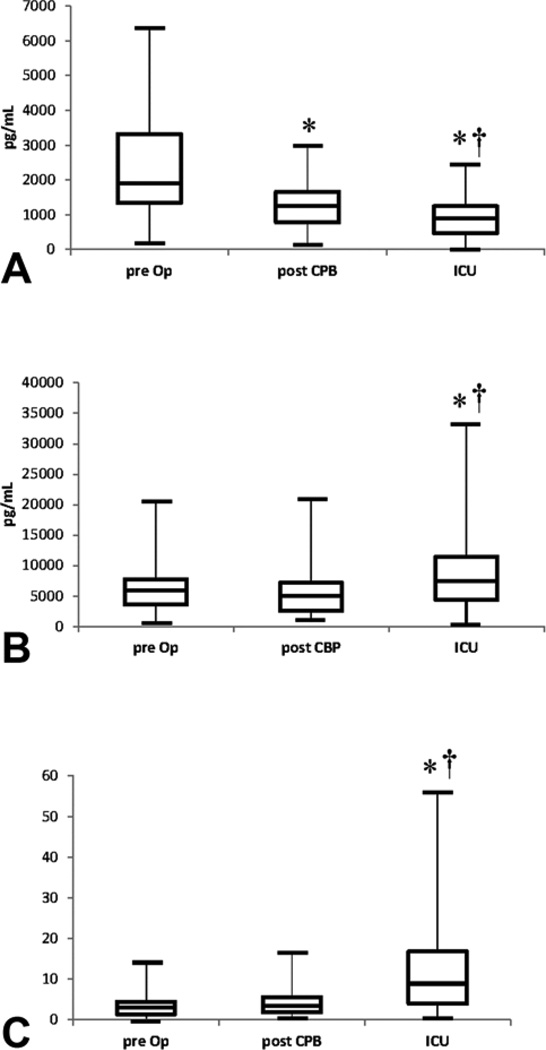
Thirty-one patients were enrolled. Angpt-1 levels significantly decreased across all time points (p<0.01). Angpt-2 concentrations were significantly elevated at intensive care unit admission when compared with both preoperative and post-cardiopulmonary bypass levels (p<0.01). The angpt-2:1 ratio significantly increased after cardiopulmonary bypass to intensive care unit admission (p<0.01). There was no significant difference between the angpt-2 or angpt-1 percentage of extraction within MUF effluent. Interleukin-8 and interleukin-10 significantly increased from preoperative to intensive care unit admission (both p<0.01).
The results of this study demonstrate that MUF removes both proinflammatory and antiinflammatory mediators equally. This study suggests that the clinical benefits of MUF cannot be attributed to the removal of larger quantities of proinflammatory mediators such as angpt-2 and interleukin-8.
体外循环会使患者血液发生血液稀释并处于非生理状态,从而引发全身炎症反应。改良超滤(MUF)可对抗血液稀释,并且还被推测可通过清除促炎细胞因子来改善预后。本研究的目的是调查MUF的益处是否包括清除促炎介质,如血管生成素-2(angpt-2)。我们假设MUF的一些临床益处与angpt-2的优先清除有关。
我们对18岁及以下接受体外循环的儿童进行了一项前瞻性队列研究。在术前、体外循环后以及重症监护病房入院时从每位患者获取血清样本。还对MUF流出液的一份液体样本进行了分析。通过酶联免疫吸附测定法测定angpt-1、angpt-2、白细胞介素-8和白细胞介素-10水平。
共纳入31例患者。angpt-1水平在所有时间点均显著下降(p<0.01)。与术前和体外循环后水平相比,重症监护病房入院时angpt-2浓度显著升高(p<0.01)。从体外循环到重症监护病房入院,angpt-2:1比值显著增加(p<0.01)。MUF流出液中angpt-2或angpt-1的提取百分比之间无显著差异。从术前到重症监护病房入院,白细胞介素-8和白细胞介素-10显著增加(均为p<0.01)。
本研究结果表明,MUF对促炎介质和抗炎介质的清除效果相同。本研究提示,MUF 的临床益处不能归因于清除了大量促炎介质,如 angpt-2 和白细胞介素-8。