Bazargani Yaser T, de Boer Anthonius, Leufkens Hubert G M, Mantel-Teeuwisse Aukje K
Division of Pharmacoepidemiology and Clinical Pharmacology, Utrecht Institute for Pharmaceutical Sciences, Utrecht University, Utrecht, the Netherlands.
PLoS One. 2014 Sep 26;9(9):e106072. doi: 10.1371/journal.pone.0106072. eCollection 2014.
Diabetes is a growing burden especially in low and middle income countries (LMICs). Inadequate access to diabetes care is of particular concern and selection of appropriate diabetes medicines on national essential medicines lists (NEMLs) is a first step in achieving adequate access. This selection was studied among LMICs and influences of various factors associated with selection decisions were assessed.
Countries were studied if they employed NEMLs for reimbursement or procurement purposes. Presence and number of essential diabetes medicines from different classes, both insulins and oral blood glucose lowering medicines, were surveyed and calculated. Data were also analyzed by country income level, geographic region, year of last update of the NEML and purpose of NEML employment. The effect of prevalence and burden of disease on the number of essential diabetes medicines was also studied. Non parametric tests and univariate linear regression analysis were used.
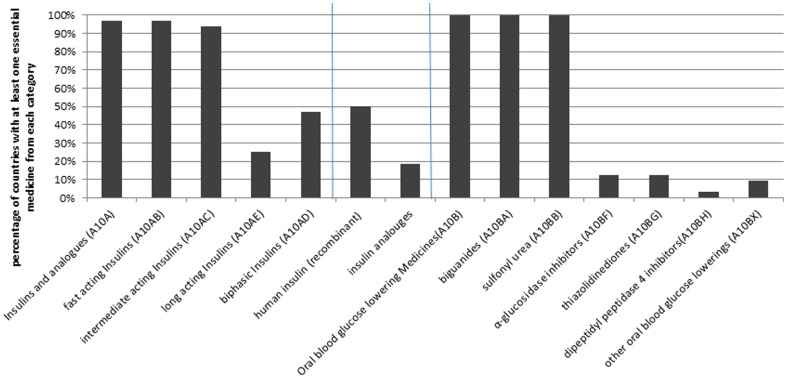
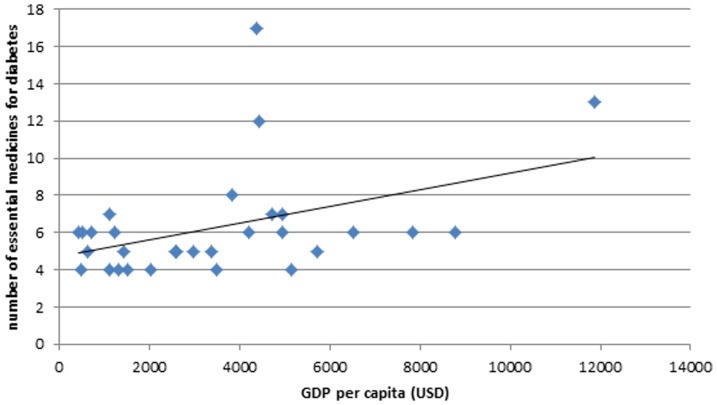
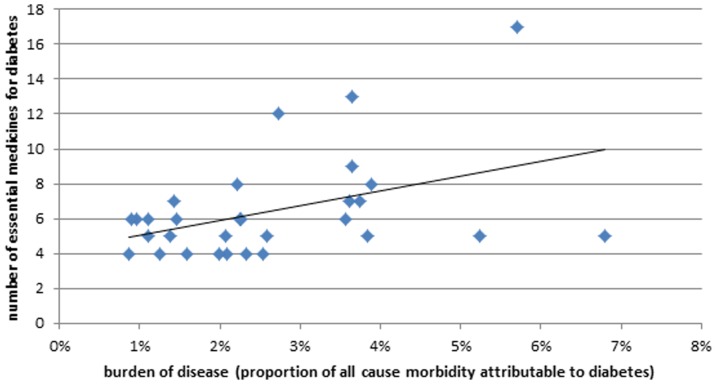
Nearly all countries (n = 32) had chosen fast (97%) and intermediate acting insulin (93%), glibenclamide and metformin (100% both) as essential medicines. The median number of essential diabetes medicines was 6, equally divided between insulins and oral medicines. 20% of the countries had selected insulin analogues as essential medicines. Among all the studied factors, an increase in burden of diabetes and wealth of countries were associated with selection of higher numbers of essential diabetes medicines (p = 0.02 in both cases).
Nearly all the studied LMICs had included the minimum required medicines for diabetes management in their NEMLs. Selection can still be improved (e.g. exclusion of insulin analogues and replacement of glibenclamide by gliclazide). Nevertheless, the known suboptimal and inconsistent availability of essential diabetes medicines in LMICs cannot be explained by inadequate selection of essential medicines. Countries should therefore be encouraged to give precedence to implementation of NEMLs to make essential diabetes medicines more accessible.
糖尿病带来的负担日益加重,在低收入和中等收入国家(LMICs)尤为如此。糖尿病护理服务难以充分获取这一问题备受关注,而在国家基本药物清单(NEMLs)中选择合适的糖尿病药物是实现充分获取的第一步。本研究针对LMICs进行了此项选择研究,并评估了与选择决策相关的各种因素的影响。
对那些将NEMLs用于报销或采购目的的国家进行研究。调查并计算了不同类别基本糖尿病药物(包括胰岛素和口服降糖药)的存在情况和数量。还按国家收入水平、地理区域、NEML的最后更新年份以及NEML的使用目的对数据进行了分析。此外,还研究了疾病患病率和负担对基本糖尿病药物数量的影响。采用了非参数检验和单变量线性回归分析。
几乎所有国家(n = 32)都选择了速效胰岛素(97%)、中效胰岛素(93%)、格列本脲和二甲双胍(两者均为100%)作为基本药物。基本糖尿病药物的中位数为6种,胰岛素和口服药物各占一半。20%的国家选择了胰岛素类似物作为基本药物。在所有研究因素中,糖尿病负担的增加和国家财富与选择更多数量的基本糖尿病药物相关(两种情况p均 = 0.02)。
几乎所有研究的LMICs在其NEMLs中都纳入了糖尿病管理所需的最低药物。选择仍有改进空间(例如排除胰岛素类似物,用格列齐特替代格列本脲)。然而,LMICs中已知的基本糖尿病药物供应不足且不一致的情况不能用基本药物选择不当来解释。因此,应鼓励各国优先实施NEMLs,以使基本糖尿病药物更容易获取。