Bazargani Y T, Ugurlu M, de Boer A, Leufkens H G M, Mantel-Teeuwisse A K
Division of Pharmacoepidemiology and Clinical Pharmacology, Utrecht Institute for Pharmaceutical Sciences, Utrecht University, PO Box 80082, 3508, TB, Utrecht, The Netherlands.
BMC Cardiovasc Disord. 2018 Jun 25;18(1):126. doi: 10.1186/s12872-018-0858-5.
The incidence and mortality of cardiovascular diseases (CVDs) in low and middle income countries (LMICs) have been increasing, while access to CVDs medicines is suboptimal. We assessed selection of essential medicines for the prevention and treatment of CVDs on national essential medicines lists (NEMLs) of LMICs and potential determinants for selection.
Only operational NEMLs were considered eligible for this study. A selection of medicines listed under "cardiovascular medicines" or "blood products and plasma substitutes" in the NEMLs were included if they were present on international guidelines for the prevention and treatment of CVDs (hyperlipidemia, hypertension, platelet inhibition, ischemic stroke, stable ischemic heart disease, acute coronary syndromes, heart failure, atrial fibrillation, peripheral arterial disease and acute limb ischemia). The number and diversity of essential medicines selected for CVDs were studied. Moreover, determinants of selection of essential medicines for CVDs at a national level were explored. Data analysis was done using univariate linear regression and non-parametric tests.
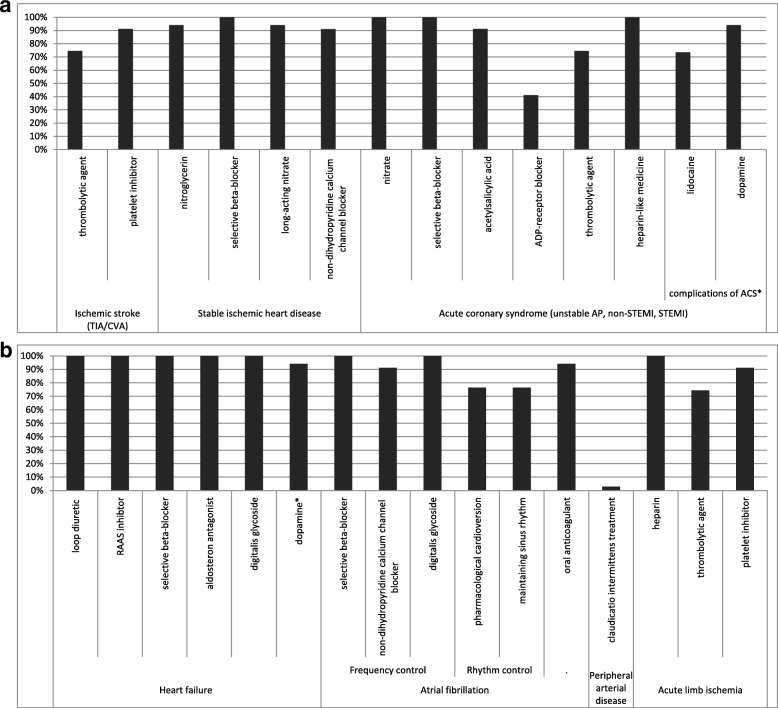
All medicine groups listed by the international guidelines were selected by the majority of the 34 countries studied with the exception of adenosine diphosphate receptor inhibitors which appeared on less than half of the NEMLs studied (41% of countries). The total number of essential medicines for the prevention and treatment of cardiovascular diseases (median 24 (range 16-50)) differed significantly across income levels (median range: 19.5-25, p = 0.014) and across regions (median range: 20-32, p = 0.049). When recommendations of the international guidelines were considered, over 75% of the NEMLs contained essential medicines for the majority of CVDs.
The main medicine classes for the management of CVDs were represented on NEMLs. Consequently, for the majority of CVDs, evidence-based guideline-recommended treatment is possible as far as selection of essential medicines is concerned. Selection will therefore not be the limiting step in access to medicines for cardiovascular diseases.
低收入和中等收入国家(LMICs)心血管疾病(CVDs)的发病率和死亡率一直在上升,而获得心血管疾病药物的情况并不理想。我们评估了低收入和中等收入国家国家基本药物清单(NEMLs)上用于预防和治疗心血管疾病的基本药物选择以及选择的潜在决定因素。
只有现行的国家基本药物清单被认为符合本研究的条件。如果国家基本药物清单中列在“心血管药物”或“血液制品和血浆代用品”项下的药物出现在心血管疾病预防和治疗的国际指南(高脂血症、高血压、血小板抑制、缺血性中风、稳定型缺血性心脏病、急性冠状动脉综合征、心力衰竭、心房颤动、外周动脉疾病和急性肢体缺血)中,则将其纳入研究。研究了所选心血管疾病基本药物的数量和多样性。此外,还探讨了国家层面心血管疾病基本药物选择的决定因素。使用单变量线性回归和非参数检验进行数据分析。
除二磷酸腺苷受体抑制剂出现在不到一半的研究国家基本药物清单中(41%的国家)外,国际指南列出的所有药物类别都被34个研究国家中的大多数所选择。预防和治疗心血管疾病的基本药物总数(中位数为24(范围为16 - 50))在不同收入水平(中位数范围:19.5 - 25,p = 0.014)和不同地区(中位数范围:20 - 32,p = 0.049)之间存在显著差异。当考虑国际指南的建议时,超过75%的国家基本药物清单包含了大多数心血管疾病的基本药物。
国家基本药物清单中体现了心血管疾病管理的主要药物类别。因此,就基本药物的选择而言,对于大多数心血管疾病,基于证据的指南推荐治疗是可行的。因此,选择不会成为获得心血管疾病药物的限制步骤。