Kahn Henry S, Gu Qiuping, Bullard Kai McKeever, Freedman David S, Ahluwalia Namanjeet, Ogden Cynthia L
Division of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia, United States of America.
Division of Health and Nutrition Examination Surveys, National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, Maryland, United States of America.
PLoS One. 2014 Oct 1;9(10):e108707. doi: 10.1371/journal.pone.0108707. eCollection 2014.
The sagittal abdominal diameter (SAD) measured in supine position is an alternative adiposity indicator that estimates the quantity of dysfunctional adipose tissue in the visceral depot. However, supine SAD's distribution and its association with health risk at the population level are unknown. Here we describe standardized measurements of SAD, provide the first, national estimates of the SAD distribution among US adults, and test associations of SAD and other adiposity indicators with prevalent dysglycemia.
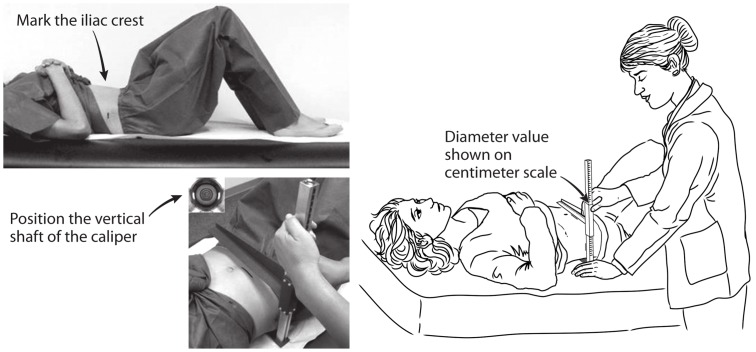
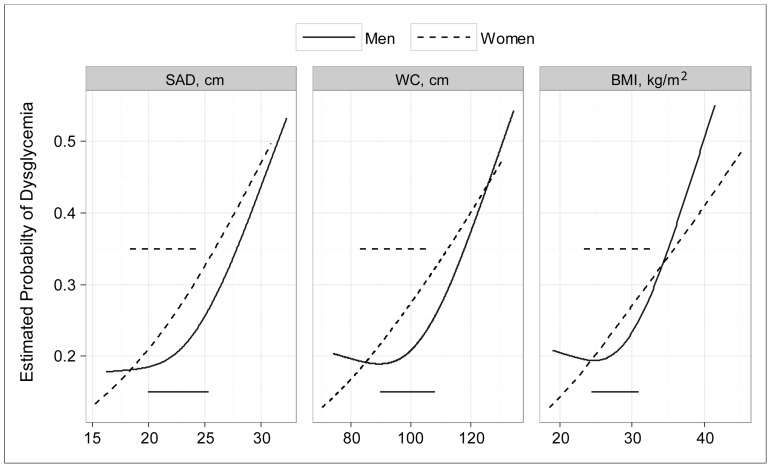
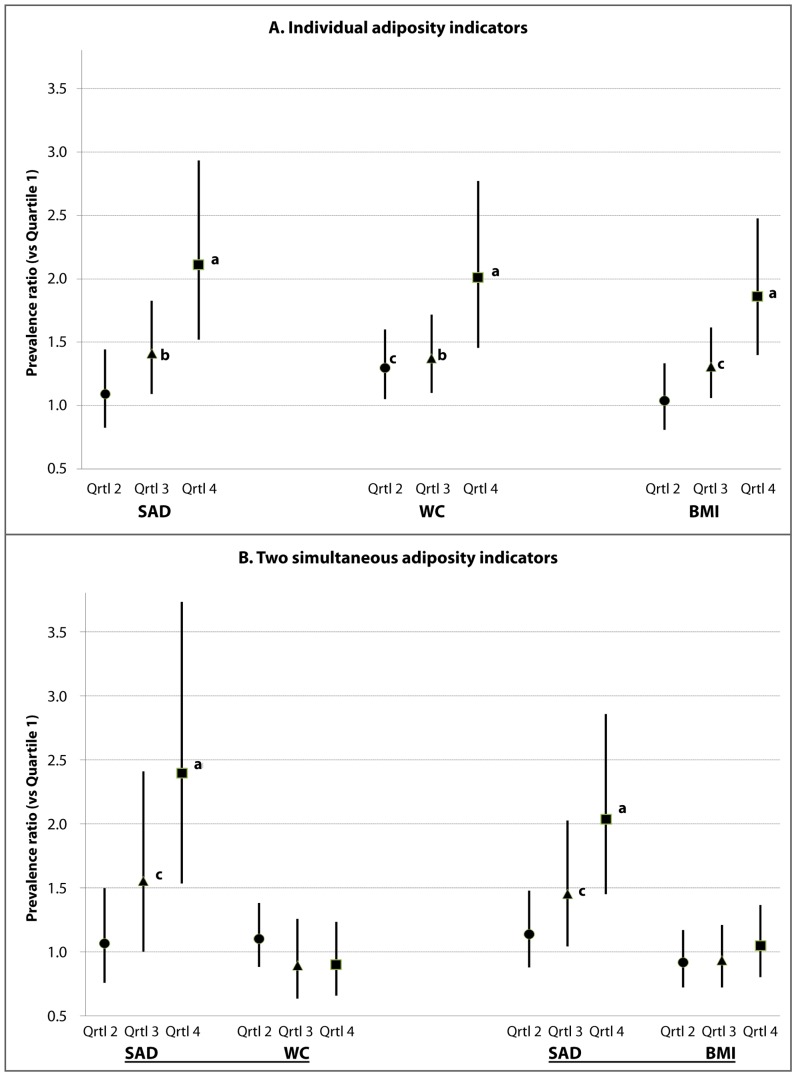
In the 2011-2012 National Health and Nutrition Examination Survey, supine SAD was measured ("abdominal height") between arms of a sliding-beam caliper at the level of the iliac crests. From 4817 non-pregnant adults (age ≥ 20; response rate 88%) we used sample weights to estimate SAD's population distribution by sex and age groups. SAD's population mean was 22.5 cm [95% confidence interval 22.2-22.8]; median was 21.9 cm [21.6-22.4]. The mean and median values of SAD were greater for men than women. For the subpopulation without diagnosed diabetes, we compared the abilities of SAD, waist circumference (WC), and body mass index (BMI, kg/m(2)) to identify prevalent dysglycemia (HbA1c ≥ 5.7%). For age-adjusted, logistic-regression models in which sex-specific quartiles of SAD were considered simultaneously with quartiles of either WC or BMI, only SAD quartiles 3 (p<0.05 vs quartile 1) and 4 (p<0.001 vs quartile 1) remained associated with increased dysglycemia. Based on continuous adiposity indicators, analyses of the area under the receiver operating characteristic curve (AUC) indicated that the dysglycemia model fit for SAD (age-adjusted) was 0.734 for men (greater than the AUC for WC, p<0.001) and 0.764 for women (greater than the AUC for WC or BMI, p<0.001).
Measured inexpensively by bedside caliper, SAD was associated with dysglycemia independently of WC or BMI. Standardized SAD measurements may enhance assessment of dysfunctional adiposity.
仰卧位测量的腹矢状径(SAD)是一种替代肥胖指标,可估计内脏脂肪库中功能失调脂肪组织的数量。然而,仰卧位SAD在人群中的分布及其与健康风险的关联尚不清楚。在此,我们描述了SAD的标准化测量方法,提供了美国成年人中SAD分布的首个全国性估计值,并测试了SAD及其他肥胖指标与糖尿病前期的关联。
在2011 - 2012年全国健康和营养检查调查中,在髂嵴水平用滑动卡尺在双臂之间测量仰卧位SAD(“腹高”)。从4817名非妊娠成年人(年龄≥20岁;应答率88%)中,我们使用样本权重按性别和年龄组估计SAD的人群分布。SAD的人群均值为22.5厘米[95%置信区间22.2 - 22.8];中位数为21.9厘米[21.6 - 22.4]。男性的SAD均值和中位数高于女性。对于未诊断出糖尿病的亚组人群,我们比较了SAD、腰围(WC)和体重指数(BMI,kg/m²)识别糖尿病前期(糖化血红蛋白≥5.7%)的能力。在年龄调整的逻辑回归模型中,将SAD的性别特异性四分位数与WC或BMI的四分位数同时考虑,只有SAD的四分位数3(与四分位数1相比,p<0.05)和4(与四分位数1相比,p<0.001)与糖尿病前期增加相关。基于连续肥胖指标,对受试者工作特征曲线(AUC)下面积的分析表明,男性SAD(年龄调整)的糖尿病前期模型拟合度为0.734(大于WC的AUC,p<0.001),女性为0.764(大于WC或BMI的AUC,p<0.001)。
通过床边卡尺廉价测量,SAD与糖尿病前期独立于WC或BMI相关。标准化的SAD测量可能会增强对功能失调性肥胖的评估。