Ohba Shinichi, Yokoyama Junkichi, Fujimaki Mitsuhisa, Kojima Masataka, Ikeda Katsuhisa
Department of Otorhinolaryngology-Head and Neck Surgery, Juntendo University School of Medicine, 2-1-1, Hongo, Bunkyo-ku, Tokyo 113-8421, Japan.
World J Surg Oncol. 2014 Oct 2;12:303. doi: 10.1186/1477-7819-12-303.
Surgery remains the main treatment for locally advanced thyroid cancers invading the trachea, esophagus, and recurrent laryngeal nerve. However, extensive resection of such tumors can sometimes involve difficulties and may result in the deterioration of the patient's quality of life. The surgeon should consider not only the patient's prognosis but also the preservation of postoperative function.
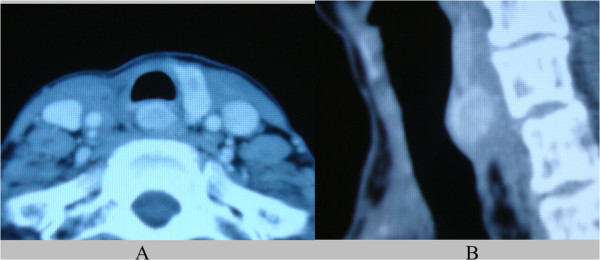
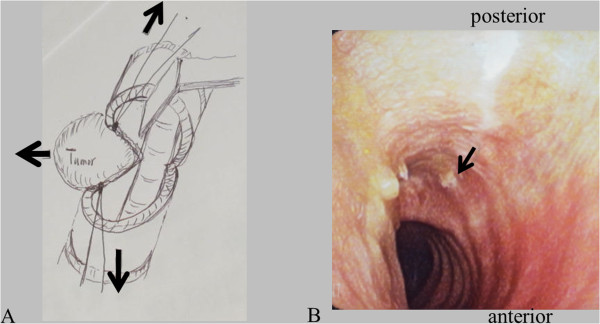
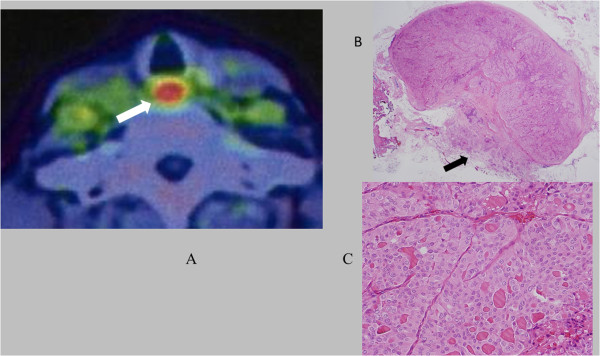
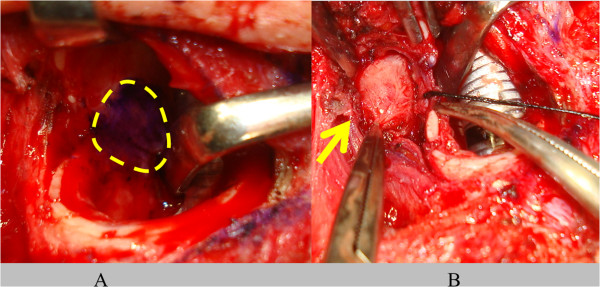
This report describes a minimally invasive surgical procedure for recurrent poorly differentiated papillary thyroid carcinoma involving the trachea and esophagus. To decrease the potential for recurrent laryngeal nerve injuries and to preserve both the tracheal and esophageal blood supply, we adapted a transtracheal approach; the recurrent tumor was safely and completely removed without causing a dysfunction. After a tracheotomy to the right, the tumor was easily detected through the tracheostoma and delineated by palpation. The mucous membrane of the trachea was minimally incised along the right-hand border of the tumor and a mucosal flap was elevated. The left side of the trachea including the membranous wall and cartilage of the tracheal mucosa was maximally preserved, to maintain the vascular supply to the trachea. Finally, the membranous wall of the trachea was preserved to within one-third of the left-hand side. Furthermore, the risk of bleeding from major lateral vessels was reduced. A sternocleidomastoid muscle flap was elevated and inserted into the cavity resulting from the tumor resection and sutured between the esophagus and trachea. The membranous wall of the tracheal mucosa was also sutured submucosally.
The tumor was removed completely with the muscular layer of the esophagus without injury to the intact recurrent laryngeal nerve and lateral major vessels. The patient started oral nutritional intake on the first postoperative day and was discharged without any significant postoperative complications.
This new procedure for transtracheal resection for recurrent thyroid cancer involving the trachea and esophagus was useful and safe.
手术仍然是侵犯气管、食管和喉返神经的局部晚期甲状腺癌的主要治疗方法。然而,此类肿瘤的广泛切除有时会遇到困难,并可能导致患者生活质量下降。外科医生不仅应考虑患者的预后,还应考虑术后功能的保留。
本报告描述了一种用于复发性低分化乳头状甲状腺癌侵犯气管和食管的微创手术方法。为了降低喉返神经损伤的可能性并保留气管和食管的血供,我们采用了经气管入路;复发性肿瘤被安全、完全地切除,且未导致功能障碍。在右侧行气管切开术后,通过气管造口很容易检测到肿瘤,并通过触诊进行描绘。沿着肿瘤的右侧边缘对气管黏膜进行最小程度的切开,并掀起一个黏膜瓣。最大限度地保留气管左侧,包括气管黏膜的膜壁和软骨,以维持气管的血供。最后,将气管膜壁保留在左侧的三分之一以内。此外,还降低了主要侧支血管出血的风险。掀起胸锁乳突肌瓣并插入肿瘤切除后形成的腔隙,缝合于食管和气管之间。气管黏膜的膜壁也进行黏膜下缝合。
肿瘤与食管肌层一并完全切除,未损伤完整的喉返神经和主要侧支血管。患者术后第一天开始经口营养摄入,出院时无任何明显的术后并发症。
这种用于复发性甲状腺癌侵犯气管和食管的经气管切除术的新方法是有用且安全的。