Mauri Tommaso, Coppadoro Andrea, Bombino Michela, Bellani Giacomo, Zambelli Vanessa, Fornari Carla, Berra Lorenzo, Bittner Edward A, Schmidt Ulrich, Sironi Marina, Bottazzi Barbara, Brambilla Paolo, Mantovani Alberto, Pesenti Antonio
Crit Care. 2014 Oct 15;18(5):562. doi: 10.1186/s13054-014-0562-5.
Timely diagnosis of pneumonia in intubated critically ill patients is rather challenging. Pentraxin 3 (PTX3) is an acute-phase mediator produced by various cell types in the lungs. Animal studies have shown that, during pneumonia, PTX3 participates in fine-tuning of inflammation (for example, microbial clearance and recruitment of neutrophils). We previously described an association between alveolar PTX3 and lung infection in a small group of intubated patients. The aim of the present study was to determine a threshold level of alveolar PTX3 with elevated sensitivity and specificity for microbiologically confirmed pneumonia.
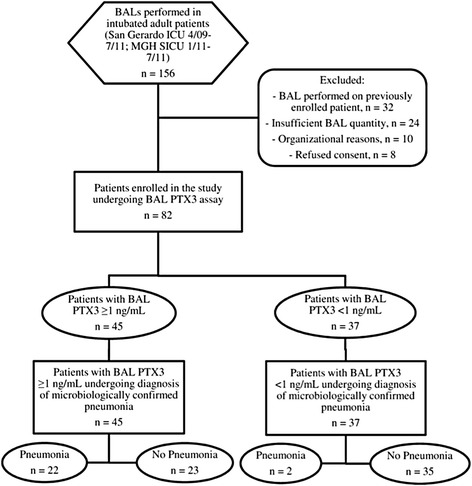
We recruited 82 intubated patients from two intensive care units (San Gerardo Hospital, Monza, Italy, and Massachusetts General Hospital, Boston, MA, USA) undergoing bronchoalveolar lavage (BAL) as per clinical decision. We collected BAL fluid and plasma samples, together with relevant clinical and microbiological data. We assayed PTX3 and soluble triggering receptor expressed on myeloid cells 1 (sTREM-1) in BAL fluid and PTX3, sTREM-1, C-reactive protein (CRP) and procalcitonin (PCT) in plasma. Two blinded independent physicians reviewed patient data to confirm pneumonia. We determined the PTX3 threshold in BAL fluid for pneumonia and compared it to other biomarkers.
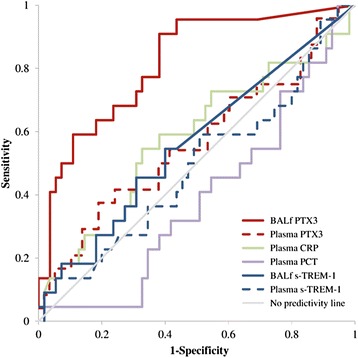
Microbiologically confirmed pneumonia of bacterial (n =12), viral (n =4) or fungal (n =8) etiology was diagnosed in 24 patients (29%). PTX3 levels in BAL fluid predicted pneumonia with an area under the receiving operator curve of 0.815 (95% CI =0.710 to 0.921, P <0.0001), whereas none of the other biomarkers were effective. In particular, PTX3 levels ≥1 ng/ml in BAL fluid predicted pneumonia in univariate analysis (β =2.784, SE =0.792, P <0.001) with elevated sensitivity (92%), specificity (60%) and negative predictive value (95%). Net reclassification index PTX3 values ≥1 ng/ml in BAL fluid for pneumonia indicated gain in sensitivity and/or specificity vs. all other mediators. These results did not change when we limited our analyses only to confirmed cases of bacterial pneumonia. Moreover, when we considered only the 70 patients who fulfilled the clinical criteria for the diagnosis of pneumonia at BAL fluid sampling, the diagnostic accuracy of PTX levels was confirmed in univariate and ROC curve analysis.
In this hypothesis-generating convenience sample, a PTX3 level ≥1 ng/ml in BAL fluid was discriminative of microbiologically confirmed pneumonia in mechanically ventilated patients.
对接受气管插管的危重症患者进行肺炎的及时诊断颇具挑战性。五聚素3(PTX3)是一种由肺内多种细胞类型产生的急性期介质。动物研究表明,在肺炎期间,PTX3参与炎症的精细调节(例如微生物清除和中性粒细胞募集)。我们之前在一小群接受气管插管的患者中描述了肺泡PTX3与肺部感染之间的关联。本研究的目的是确定肺泡PTX3的阈值水平,以提高对微生物学确诊肺炎的敏感性和特异性。
我们从两个重症监护病房(意大利蒙扎的圣杰拉尔多医院和美国马萨诸塞州波士顿的麻省总医院)招募了82名接受气管插管的患者,这些患者根据临床决策接受支气管肺泡灌洗(BAL)。我们收集了BAL液和血浆样本,以及相关的临床和微生物学数据。我们检测了BAL液中的PTX3和髓系细胞表面表达的可溶性触发受体1(sTREM-1),以及血浆中的PTX3、sTREM-1、C反应蛋白(CRP)和降钙素原(PCT)。两名盲法独立医生审查患者数据以确诊肺炎。我们确定了BAL液中肺炎的PTX3阈值,并将其与其他生物标志物进行比较。
在24名患者(29%)中诊断出微生物学确诊的细菌性(n =12)、病毒性(n =4)或真菌性(n =8)肺炎。BAL液中的PTX3水平预测肺炎的受试者工作特征曲线下面积为0.815(95%CI =0.710至0.921,P <0.0001),而其他生物标志物均无效。特别是,在单变量分析中,BAL液中PTX3水平≥1 ng/ml预测肺炎(β =2.784,SE =0.792,P <0.001),敏感性(92%)、特异性(60%)和阴性预测值(95%)均升高。BAL液中肺炎的PTX3值≥1 ng/ml的净重新分类指数表明与所有其他介质相比,敏感性和/或特异性有所提高。当我们仅将分析限于确诊的细菌性肺炎病例时,这些结果没有改变。此外,当我们仅考虑在BAL液采样时符合肺炎诊断临床标准的70名患者时,PTX水平的诊断准确性在单变量和ROC曲线分析中得到证实。
在这个产生假设的便利样本中,BAL液中PTX3水平≥1 ng/ml可区分机械通气患者微生物学确诊的肺炎。