Mikami Yoko, Kolman Louis, Joncas Sebastien X, Stirrat John, Scholl David, Rajchl Martin, Lydell Carmen P, Weeks Sarah G, Howarth Andrew G, White James A
Stephenson Cardiac Imaging Centre at the Libin Cardiovascular Institute of Alberta, University of Calgary, Calgary, AB, Canada.
Imaging Research Laboratory - Robarts Research Institute, Western University, London, ON, Canada.
J Cardiovasc Magn Reson. 2014 Oct 7;16(1):85. doi: 10.1186/s12968-014-0085-x.
The presence and extent of late gadolinium enhancement (LGE) has been associated with adverse events in patients with hypertrophic cardiomyopathy (HCM). Signal intensity (SI) threshold techniques are routinely employed for quantification; Full-Width at Half-Maximum (FWHM) techniques are suggested to provide greater reproducibility than Signal Threshold versus Reference Mean (STRM) techniques, however the accuracy of these approaches versus the manual assignment of optimal SI thresholds has not been studied. In this study, we compared all known semi-automated LGE quantification techniques for accuracy and reproducibility among patients with HCM.
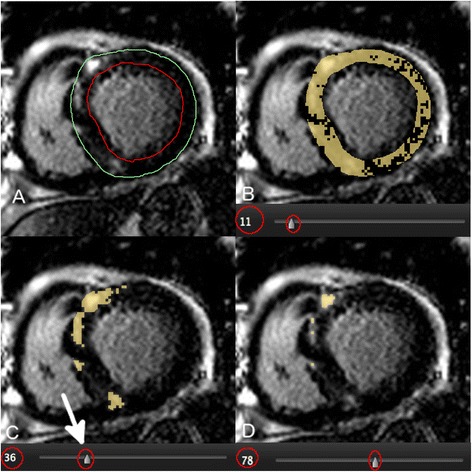
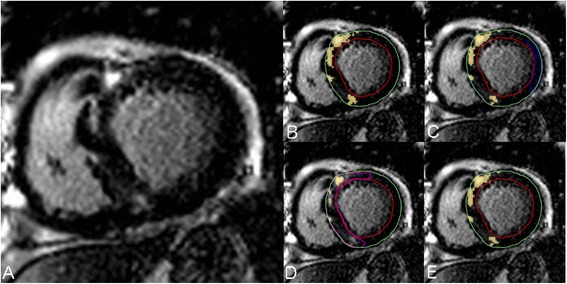
Seventy-six HCM patients (51 male, age 54 ± 13 years) were studied. Total LGE volume was quantified using 7 semi-automated techniques and compared to expert manual adjustment of the SI threshold to achieve optimal segmentation. Techniques tested included STRM based thresholds of >2, 3, 4, 5 and 6 SD above mean SI of reference myocardium, the FWHM technique, and the Otsu-auto-threshold (OAT) technique. The SI threshold chosen by each technique was recorded for all slices. Bland-Altman analysis and intra-class correlation coefficients (ICC) were reported for each semi-automated technique versus expert, manually adjusted LGE segmentation. Intra- and inter-observer reproducibility assessments were also performed.
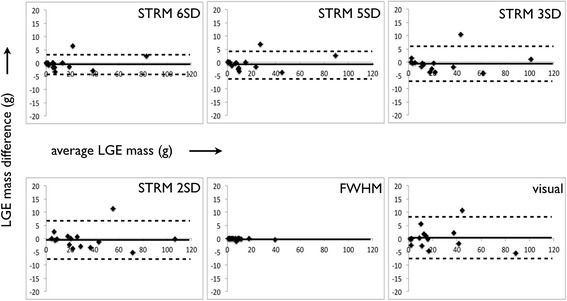
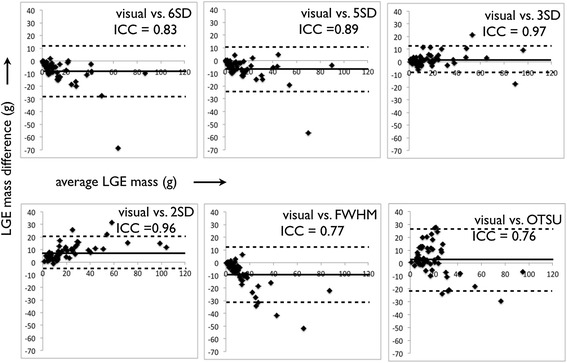
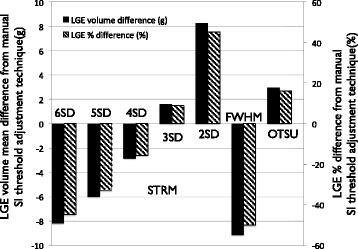
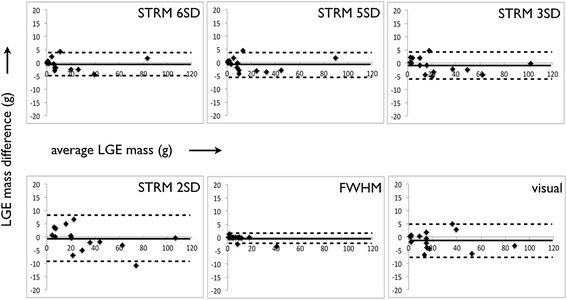
Fifty-two of 76 (68%) patients showed LGE on a total of 202 slices. For accuracy, the STRM >3SD technique showed the greatest agreement with manual segmentation (ICC = 0.97, mean difference and 95% limits of agreement = 1.6 ± 10.7 g) while STRM >6SD, >5SD, 4SD and FWHM techniques systematically underestimated total LGE volume. Slice based analysis of selected SI thresholds similarly showed the STRM >3SD threshold to most closely approximate manually adjusted SI thresholds (ICC = 0.88). For reproducibility, the intra- and inter-observer reproducibility of the >3SD threshold demonstrated an acceptable mean difference and 95% limits of agreement of -0.5 ± 6.8 g and -0.9 ± 5.6 g, respectively.
FWHM segmentation provides superior reproducibility, however systematically underestimates total LGE volume compared to manual segmentation in patients with HCM. The STRM >3SD technique provides the greatest accuracy while retaining acceptable reproducibility and may therefore be a preferred approach for LGE quantification in this population.
晚期钆增强(LGE)的存在及范围与肥厚型心肌病(HCM)患者的不良事件相关。信号强度(SI)阈值技术通常用于定量分析;建议半高宽(FWHM)技术比信号阈值与参考均值(STRM)技术具有更高的可重复性,然而,与手动设定最佳SI阈值相比,这些方法的准确性尚未得到研究。在本研究中,我们比较了所有已知的半自动LGE定量技术在HCM患者中的准确性和可重复性。
研究了76例HCM患者(51例男性,年龄54±13岁)。使用7种半自动技术对总LGE体积进行定量,并与专家手动调整SI阈值以实现最佳分割的结果进行比较。测试的技术包括基于STRM的高于参考心肌平均SI的2、3、4、5和6个标准差的阈值、FWHM技术和大津自动阈值(OAT)技术。记录所有切片上每种技术选择的SI阈值。报告每种半自动技术与专家手动调整的LGE分割之间的Bland-Altman分析和组内相关系数(ICC)。还进行了观察者内和观察者间的可重复性评估。
76例患者中有52例(68%)在总共202个切片上显示LGE。在准确性方面,STRM>3SD技术与手动分割的一致性最高(ICC = 0.97,平均差异和95%一致性界限 = 1.6±10.7 g),而STRM>6SD、>5SD、4SD和FWHM技术系统性地低估了总LGE体积。对选定SI阈值的切片分析同样显示,STRM>3SD阈值最接近手动调整的SI阈值(ICC = 0.88)。在可重复性方面,>3SD阈值的观察者内和观察者间可重复性分别显示出可接受的平均差异和95%一致性界限,分别为-0.5±6.8 g和-0.9±5.6 g。
FWHM分割提供了更高的可重复性,然而,与HCM患者的手动分割相比,系统性地低估了总LGE体积。STRM>3SD技术提供了最高的准确性,同时保持了可接受的可重复性,因此可能是该人群LGE定量的首选方法。