Hackl Christina, Popp Felix C, Ehehalt Katharina, Dendl Lena-Marie, Benseler Volker, Renner Philipp, Loss Martin, Dolderer Jurgen, Prantl Lukas, Kühnel Thomas, Schlitt Hans J, Dahlke Marc H
Department of Surgery, University Medical Center Regensburg, Regensburg 93042, Germany.
BMC Surg. 2014 Oct 15;14:78. doi: 10.1186/1471-2482-14-78.
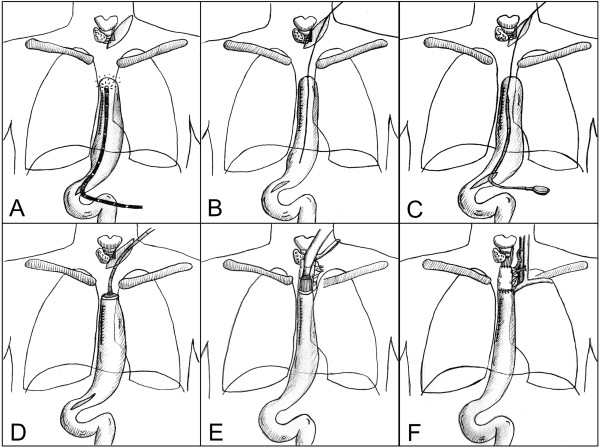
Free jejunal interposition is a useful technique for reconstruction of the cervical esophagus. However, the distal anastomosis between the graft and the remaining thoracic esophagus or a gastric conduit can be technically challenging when located very low in the thoracic aperture. We here describe a modified technique for retrograde stapling of a jejunal graft to a failed gastric conduit using a circular stapler on a delivery system.
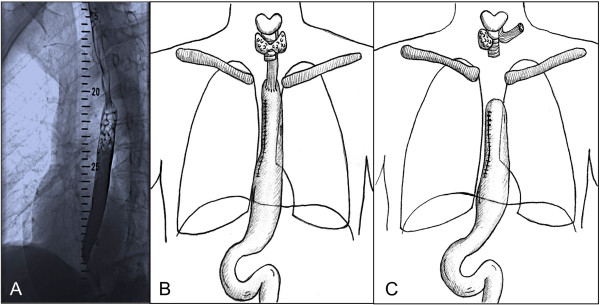
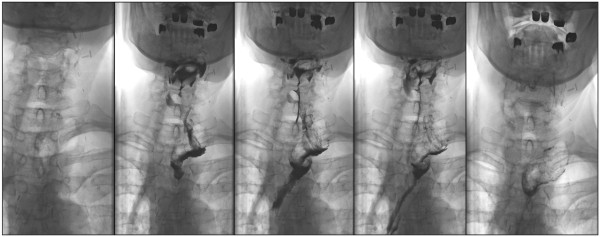
A 56 year-old patient had been referred for esophageal squamous cell carcinoma at 20 cm from the incisors. On day 8 after thoracoabdominal esophagectomy with gastric pull-up, an anastomotic leakage was diagnosed. A proximal-release stent was successfully placed by gastroscopy and the patient was discharged. Two weeks later, an esophagotracheal fistula occurred proximal to the esophageal stent. Cervical esophagostomy was performed with cranial closure of the gastric conduit, which was left in situ within the right hemithorax. Three months later, reconstruction was performed using a free jejunal interposition. The anvil of a circular stapler (Orvil®, Covidien) was placed transabdominally through an endoscopic rendez-vous procedure into the gastric conduit. A free jejunal graft was retrogradely stapled to the proximal end of the conduit. Microvascular anastomoses were performed subsequently. The proximal anastomosis of the conduit was completed manually after reperfusion.
This modified technique allows stapling of a jejunal interposition graft located deep in the thoracic aperture and is therefore a useful method that may help to avoid reconstruction by colonic pull-up and thoracotomy.
游离空肠移植术是重建颈段食管的一种有效技术。然而,当移植肠段与剩余胸段食管或胃代食管在胸廓入口处的吻合位置非常低时,技术上可能具有挑战性。我们在此描述一种改良技术,即在输送系统上使用圆形吻合器将空肠移植肠段逆行吻合至失败的胃代食管。
一名56岁患者因距门齿20 cm处的食管鳞状细胞癌前来就诊。在经胸腹联合食管切除并胃上提术后第8天,诊断出吻合口漏。通过胃镜成功置入近端释放支架,患者出院。两周后,在食管支架近端发生食管气管瘘。进行了颈段食管造口术,并将胃代食管在头侧关闭,胃代食管留在右半胸内原位。三个月后,采用游离空肠移植术进行重建。通过内镜会师操作经腹将圆形吻合器(柯惠公司的Orvil®)的钉砧置入胃代食管。将游离的空肠移植肠段逆行吻合至胃代食管的近端。随后进行微血管吻合。再灌注后手动完成胃代食管的近端吻合。
这种改良技术能够对位于胸廓入口深处的空肠移植肠段进行吻合,因此是一种有用的方法,可能有助于避免结肠上提和开胸重建。