Department of Surgery, University of California San Francisco, San Francisco, CA, USA.
Eur J Cardiothorac Surg. 2010 Jun;37(6):1421-6. doi: 10.1016/j.ejcts.2010.01.010. Epub 2010 Feb 12.
In expert hands, the intrathoracic oesophago-gastric anastamosis usually provides a low rate of strictures and leaks. However, anastomoses can be technically challenging and time consuming when minimally invasive techniques are used. We present our preliminary results of a standardised 25 mm/4.8mm circular-stapled anastomosis using a trans-orally placed anvil.
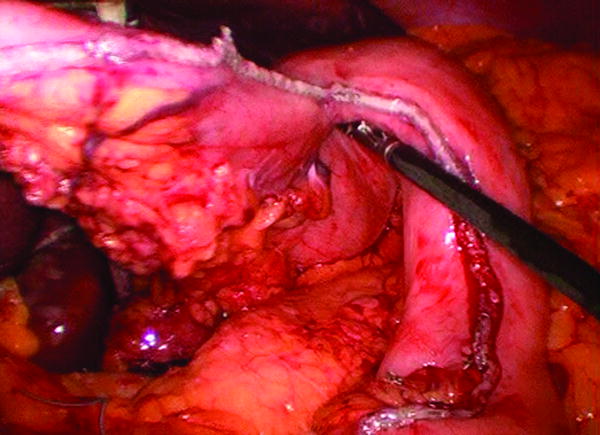
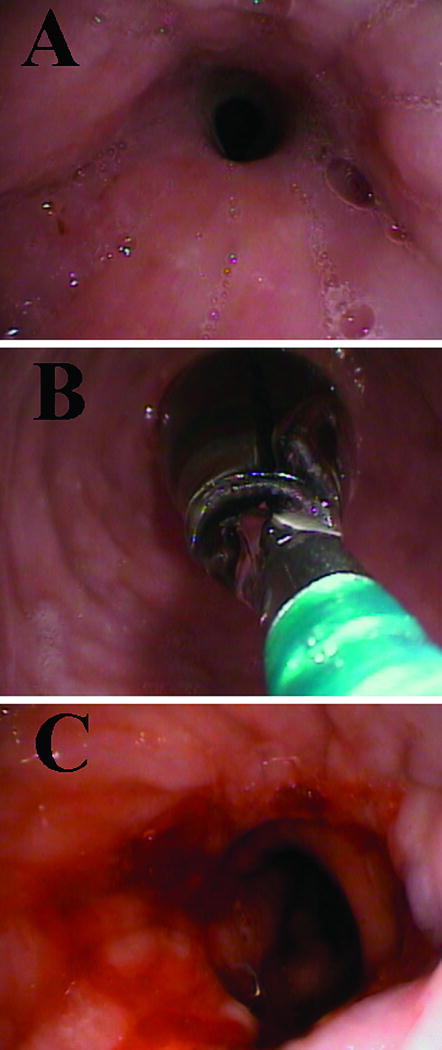
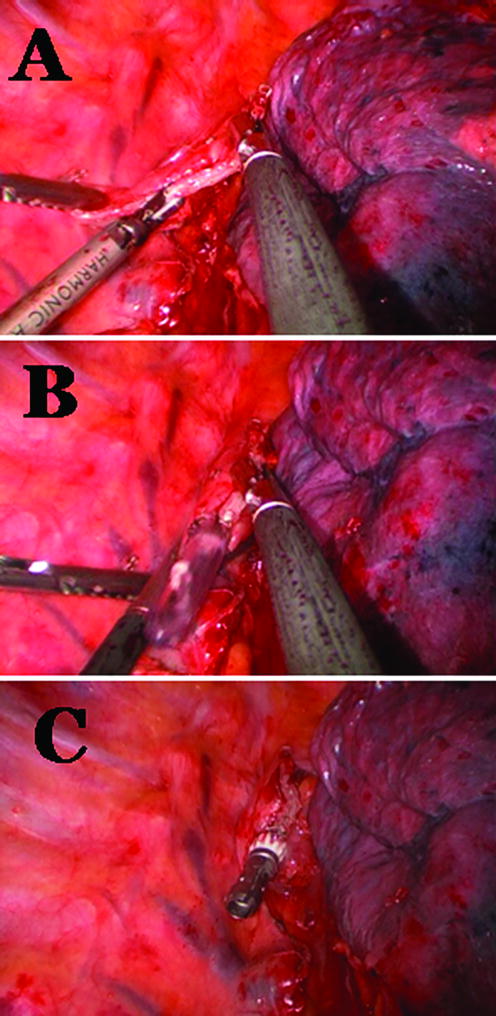
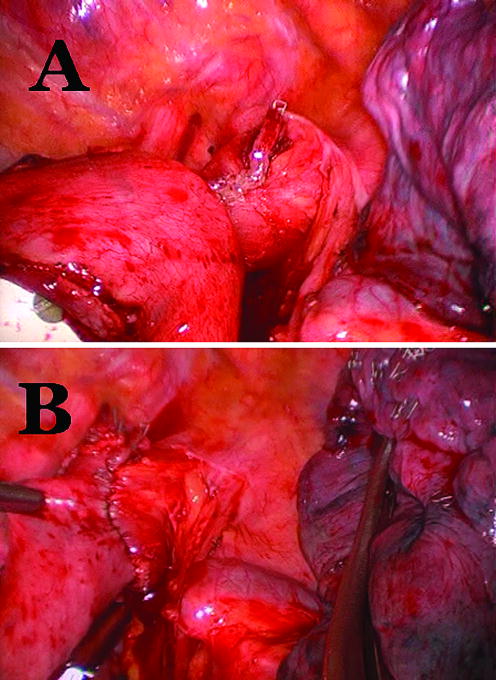
We evaluated a prospective cohort of 37 consecutive patients offered minimally invasive Ivor Lewis oesophagectomy at a tertiary referral centre. The oesophago-gastric anastomosis was created using a 25-mm anvil (Orvil, Autosuture, Norwalk, CT, USA) passed trans-orally, in a tilted position, and connected to a 90-cm long polyvinyl chloride delivery tube through an opening in the oesophageal stump. The anastomosis was completed by joining the anvil to a circular stapler (end-to-end anastomosis stapler (EEA XL) 25 mm with 4.8-mm staples, Autosuture, Norwalk, CT, USA) inserted into the gastric conduit. Primary outcomes were leak and stricture rates.
Thirty-seven patients (mean age 65 years) with distal oesophageal adenocarcinoma (n=29), squamous cell cancer (n=5) or high-grade dysplasia in Barrett's oesophagus (n=3) underwent an Ivor Lewis oesophagectomy between October 2007 and August 2009. The abdominal portion was operated laparoscopically in 30 patients (81.1%). The thoracic portion was done using a muscle-sparing mini-thoracotomy in 23 patients (62.2%) and thoracoscopic techniques in 14 patients (37.8%). There were no intra-operative technical failures of the anastomosis or deaths. Five patients had strictures (13.5%) and all were successfully treated with endoscopic dilations. One patient had an anastomotic leak (2.7%) that was successfully treated by re-operation and endoscopic stenting of the anastomosis.
The circular-stapled anastomosis with the trans-oral anvil allows for an efficient, safe and reproducible anastomosis. This straightforward technique is particularly suited to the completely minimally invasive Ivor Lewis oesophagectomy.
在专家手中,胸内食管-胃吻合术通常具有较低的狭窄和渗漏率。然而,当使用微创技术时,吻合术可能在技术上具有挑战性且耗时。我们展示了使用经口放置的吻合器进行标准化 25mm/4.8mm 圆形吻合的初步结果。
我们评估了在一家三级转诊中心接受微创 Ivor Lewis 食管切除术的 37 例连续患者的前瞻性队列。使用经口放置的 25mm 吻合器(Orvil,Autosuture,Norwalk,CT,美国)以倾斜位置穿过食管残端,将食管-胃吻合术创建,并用 90cm 长的聚氯乙烯输送管通过食管残端的开口连接。通过将吻合器连接到插入胃管的圆形吻合器(端端吻合吻合器(EEA XL)25mm 带 4.8mm 吻合钉,Autosuture,Norwalk,CT,美国)来完成吻合。主要结局是漏和狭窄的发生率。
37 例(平均年龄 65 岁)患者患有远端食管腺癌(n=29)、鳞状细胞癌(n=5)或 Barrett 食管高级别异型增生(n=3)接受了 Ivor Lewis 食管切除术,时间为 2007 年 10 月至 2009 年 8 月。30 例患者(81.1%)采用腹腔镜进行腹部手术。23 例患者(62.2%)采用肌保护微创小开胸术进行胸部手术,14 例患者(37.8%)采用胸腔镜技术进行手术。吻合术无术中技术失败或死亡。5 例患者出现狭窄(13.5%),均经内镜扩张成功治疗。1 例患者出现吻合口漏(2.7%),通过再次手术和内镜支架置入吻合口成功治疗。
经口吻合器的圆形吻合术可实现高效、安全且可重复的吻合。这种直截了当的技术特别适合完全微创的 Ivor Lewis 食管切除术。