Sun Dong, Eirin Alfonso, Zhu Xiang-Yang, Zhang Xin, Crane John A, Woollard John R, Lerman Amir, Lerman Lilach O
1] Division of Nephrology and Hypertension, Mayo Clinic, Rochester, Minnesota, USA [2] Department of Nephrology, The Affiliated Hospital of Xuzhou Medical College, Xuzhou, China.
Division of Nephrology and Hypertension, Mayo Clinic, Rochester, Minnesota, USA.
Kidney Int. 2015 Apr;87(4):719-27. doi: 10.1038/ki.2014.343. Epub 2014 Oct 22.
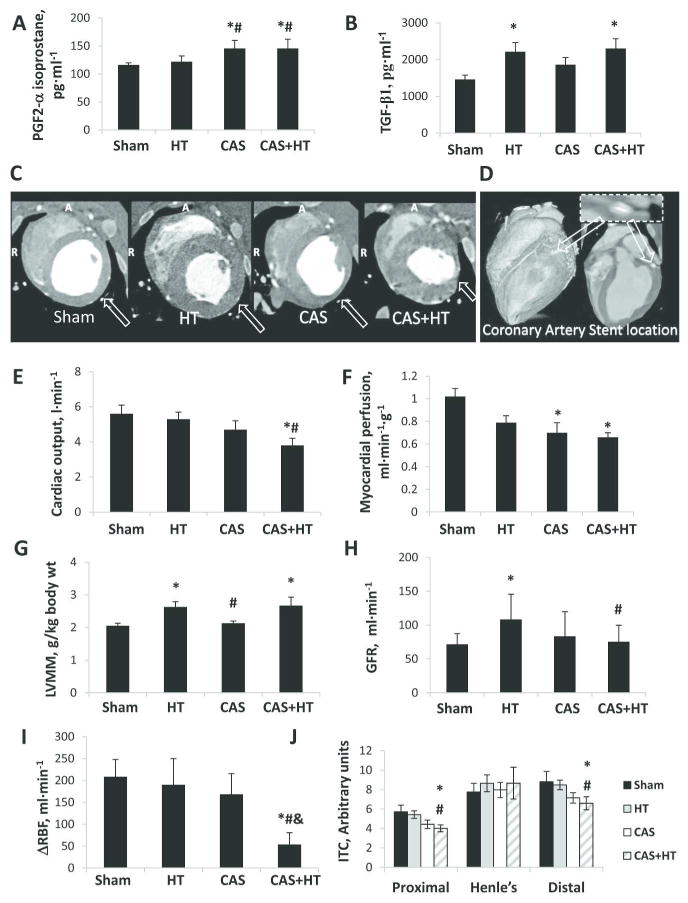
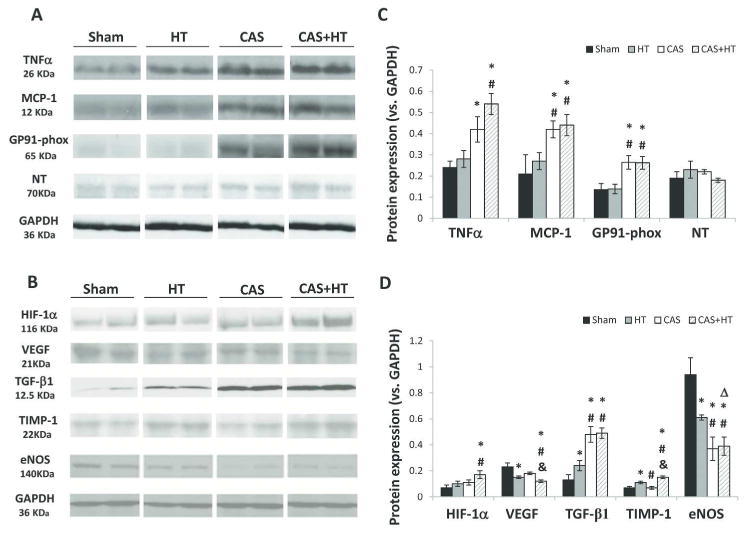
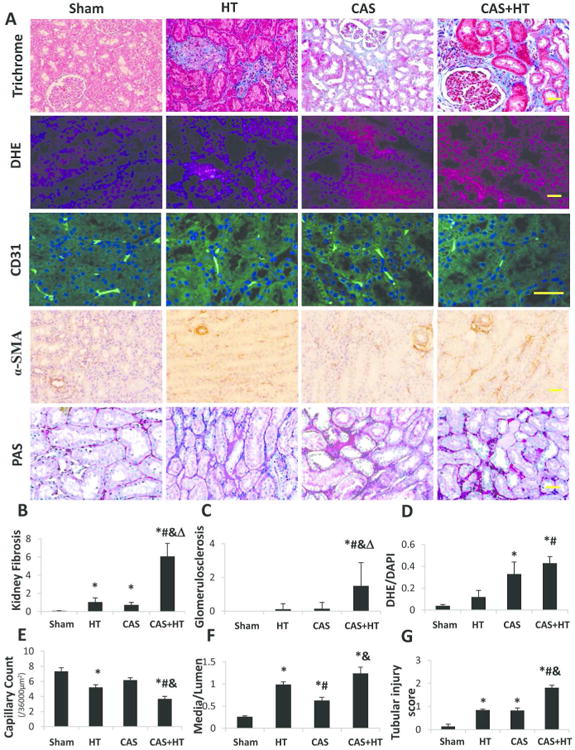
The impact of coronary artery stenosis (CAS) on renal injury is unknown. Here we tested whether the existence of CAS, regardless of concurrent atherosclerosis, would induce kidney injury and magnify its susceptibility to damage from coexisting hypertension (HT). Pigs (seven each) were assigned to sham, left-circumflex CAS, renovascular HT, and CAS plus HT groups. Cardiac and nonstenotic kidney functions, circulating and renal inflammatory and oxidative markers, and renal and microvascular remodeling were assessed 10 weeks later. Myocardial perfusion declined distal to CAS. Systemic levels of PGF2-α isoprostane, a marker of oxidative stress, increased in CAS and CAS plus HT, whereas single-kidney blood flow responses to acetylcholine were significantly blunted only in CAS plus HT compared with sham, HT, and CAS, indicating renovascular endothelial dysfunction. Tissue expression of inflammatory and oxidative markers were elevated in the CAS pig kidney, and further magnified in CAS plus HT, whereas angiogenic factor expression was decreased. Bendavia, a mitochondria-targeted peptide, decreased oxidative stress and improved renal function and structure in CAS. Furthermore, CAS and HT synergistically amplified glomerulosclerosis and renal fibrosis. Thus, mild myocardial ischemia, independent of systemic atherosclerosis, induced renal injury, possibly mediated by increased oxidative stress. Superimposed HT aggravates renal inflammation and endothelial dysfunction caused by CAS, and synergistically promotes kidney fibrosis, providing impetus to preserve cardiac integrity in order to protect the kidney.
冠状动脉狭窄(CAS)对肾损伤的影响尚不清楚。在此,我们测试了无论是否并发动脉粥样硬化,CAS的存在是否会诱发肾损伤并增加其对共存高血压(HT)损伤的易感性。将猪(每组7只)分为假手术组、左旋支冠状动脉狭窄组、肾血管性高血压组和冠状动脉狭窄加高血压组。10周后评估心脏和非狭窄肾脏功能、循环和肾脏炎症及氧化标志物以及肾脏和微血管重塑情况。冠状动脉狭窄远端的心肌灌注下降。氧化应激标志物PGF2-α异前列腺素的全身水平在冠状动脉狭窄组和冠状动脉狭窄加高血压组中升高,而与假手术组、高血压组和冠状动脉狭窄组相比,仅在冠状动脉狭窄加高血压组中,单肾血流对乙酰胆碱的反应明显减弱,表明肾血管内皮功能障碍。冠状动脉狭窄猪肾中炎症和氧化标志物的组织表达升高,在冠状动脉狭窄加高血压组中进一步放大,而血管生成因子表达降低。线粒体靶向肽Bendavia可降低氧化应激并改善冠状动脉狭窄组的肾功能和结构。此外,冠状动脉狭窄和高血压协同放大肾小球硬化和肾纤维化。因此,与全身性动脉粥样硬化无关的轻度心肌缺血可诱发肾损伤,可能由氧化应激增加介导。叠加的高血压会加重冠状动脉狭窄引起的肾脏炎症和内皮功能障碍,并协同促进肾纤维化,这为保护心脏完整性以保护肾脏提供了动力。