Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People's Republic of China.
Department of Pathology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People's Republic of China.
Onco Targets Ther. 2014 Oct 16;7:1891-9. doi: 10.2147/OTT.S67812. eCollection 2014.
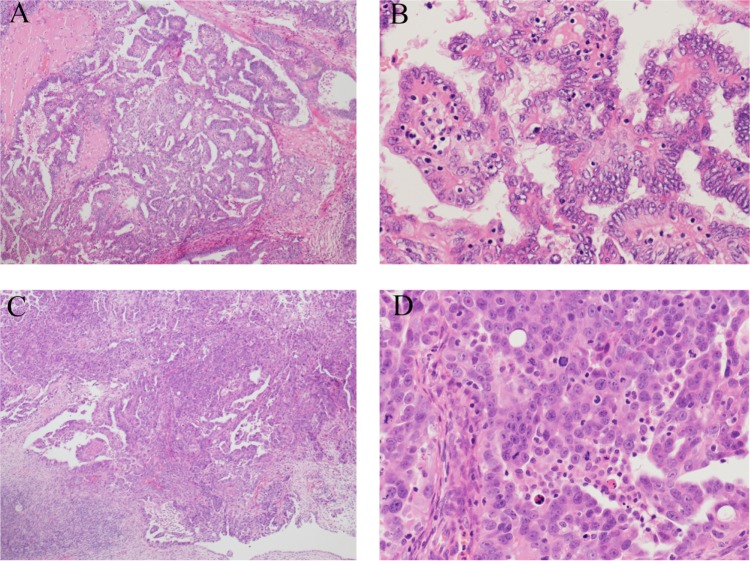
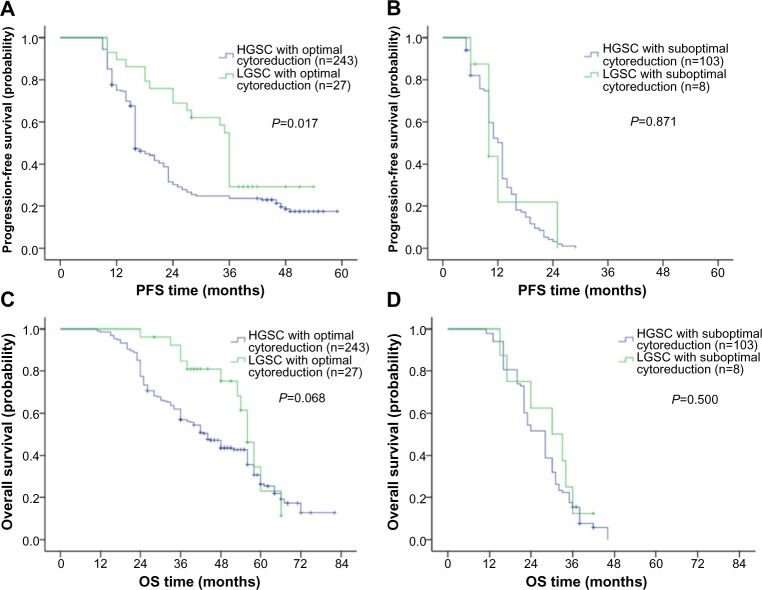
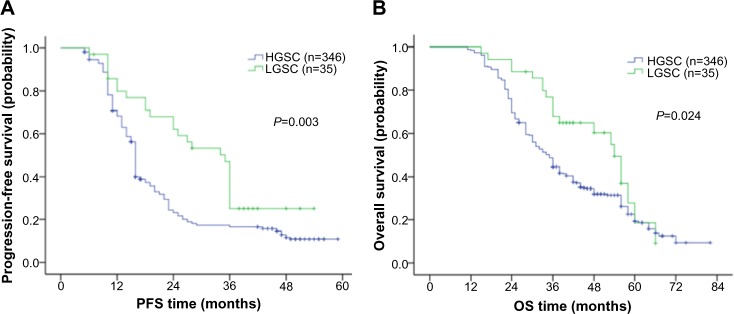
Ovarian low-grade serous carcinoma (LGSC) and high-grade serous carcinoma have distinct molecular profiles, clinical behaviors, and treatment responses. The survival advantage for patients with low-grade carcinoma compared with patients with high-grade histology remains controversial. We retrospectively reviewed the medical charts of 381 patients with ovarian serous carcinoma at Peking Union Medical College Hospital from 2007 to 2010. Patients were classified into two groups according to MD Anderson two-tier system: 35 (9.2%) cases with LGSC and 346 with high-grade serous carcinoma. Patients with low-grade serous ovarian cancer had a significantly younger age at diagnosis (46 versus 56 years, P=0.046), and their median progression-free survival (PFS) and overall survival values were 35.0 and 54.0 months, respectively. A multivariate analysis showed that, for serous ovarian cancer, the histological grade was a significant prognostic factor for PFS but not for overall survival (P=0.022 and P=0.0566, respectively). When stratified by the existence of a residual disease, patients with low-grade disease who underwent cytoreductive surgery without macroscopic residual disease (>1 cm) had a significantly improved median PFS time (36.0 months) compared with that of patients with high-grade carcinoma who received optimal cytoreductive surgery (16.0 months, P=0.017). Conversely, patients with low-grade and high-grade carcinoma who were left with macroscopic residue (>1 cm) experienced a similarly shorter median PFS (10.0 and 13.0 months, respectively, P=0.871). The International Federation of Gynecology and Obstetrics stage and residual disease were significant prognostic factors of low-grade carcinoma, while positive ascites was associated with a worse PFS value. Our data showed that LGSC is a different entity from high-grade carcinoma and that LGSC was associated with improved PFS after optimal cytoreductive surgery but not suboptimal operation.
卵巢低级别浆液性癌 (LGSC) 和高级别浆液性癌具有明显不同的分子谱、临床行为和治疗反应。与高级别组织学相比,低级别癌患者的生存优势仍存在争议。我们回顾性分析了 2007 年至 2010 年北京协和医学院医院 381 例卵巢浆液性癌患者的病历。根据 MD 安德森双层系统,患者分为两组:35 例(9.2%)LGSC 和 346 例高级别浆液性癌。低级别浆液性卵巢癌患者的诊断年龄明显更年轻(46 岁 vs 56 岁,P=0.046),中位无进展生存期(PFS)和总生存期分别为 35.0 个月和 54.0 个月。多因素分析显示,对于浆液性卵巢癌,组织学分级是 PFS 的显著预后因素,但不是总生存期的预后因素(P=0.022 和 P=0.0566)。按有无残留疾病分层,接受无肉眼残留疾病(>1 cm)的肿瘤细胞减灭术的低级别疾病患者中位 PFS 时间(36.0 个月)明显长于接受最佳肿瘤细胞减灭术的高级别癌患者(16.0 个月,P=0.017)。相反,残留疾病肉眼可见(>1 cm)的低级别和高级别癌患者的中位 PFS 时间相似(分别为 10.0 个月和 13.0 个月,P=0.871)。国际妇产科联合会(FIGO)分期和残留疾病是低级别癌的显著预后因素,而阳性腹水与较差的 PFS 值相关。我们的数据表明,LGSC 是一种与高级别癌不同的实体,在接受最佳肿瘤细胞减灭术治疗后,LGSC 与改善的 PFS 相关,但与非最佳手术无关。