Moni Mohammad Ali, Liò Pietro
Computer Laboratory, University of Cambridge, William Gates Building, 15 JJ Thomson Avenue, Cambridge CB3 0FD, UK.
BMC Bioinformatics. 2014 Oct 24;15(1):333. doi: 10.1186/1471-2105-15-333.
Infections are often associated to comorbidity that increases the risk of medical conditions which can lead to further morbidity and mortality. SARS is a threat which is similar to MERS virus, but the comorbidity is the key aspect to underline their different impacts. One UK doctor says "I'd rather have HIV than diabetes" as life expectancy among diabetes patients is lower than that of HIV. However, HIV has a comorbidity impact on the diabetes.
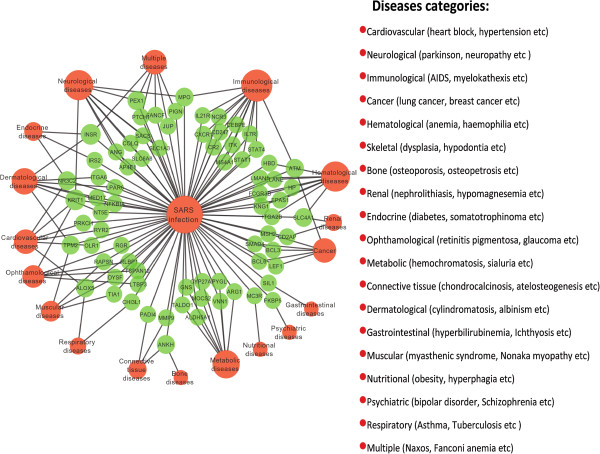
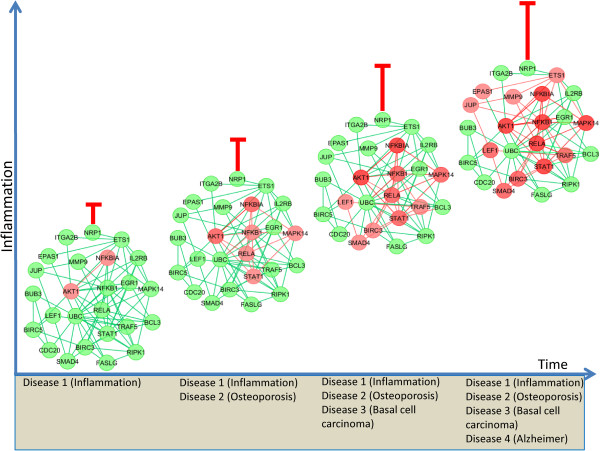
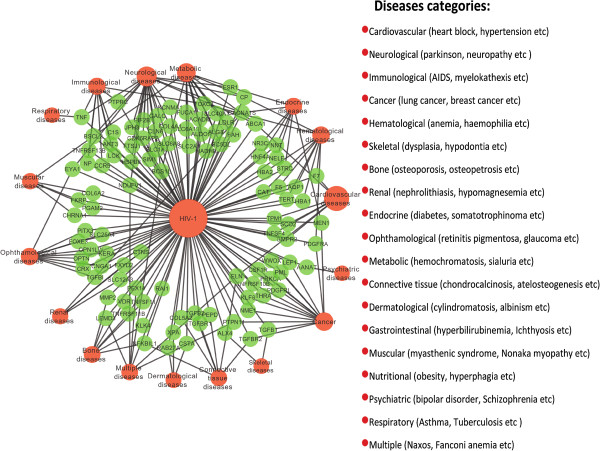
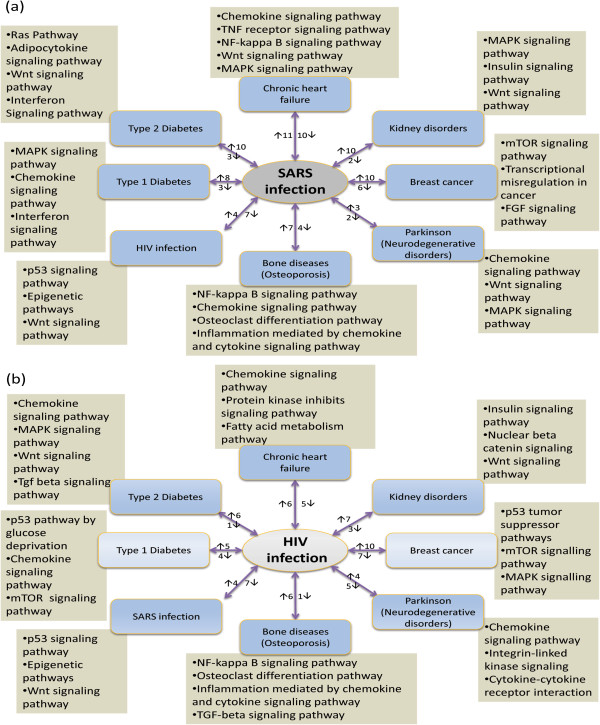
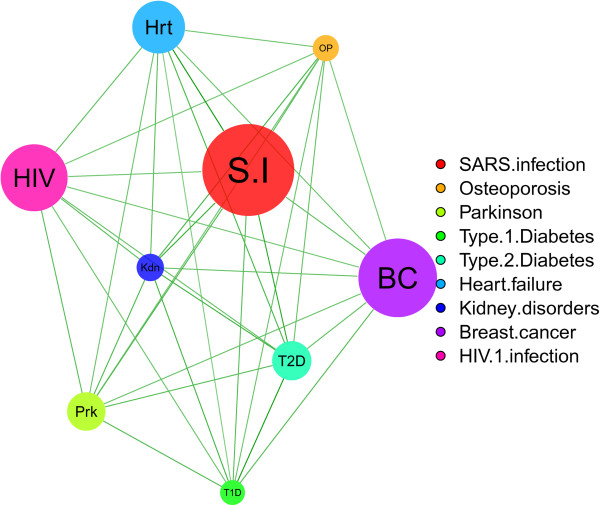
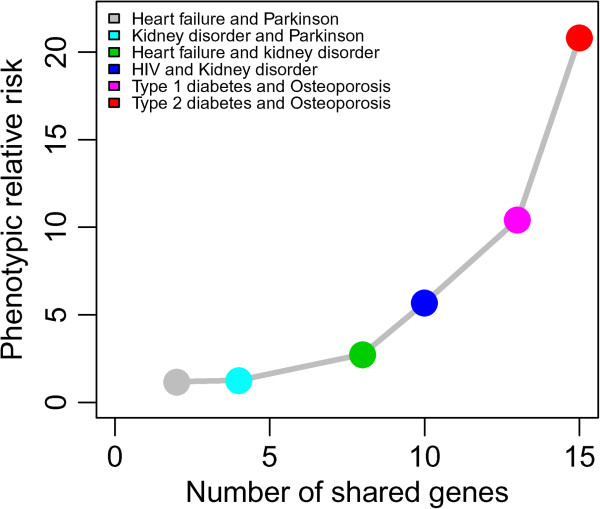
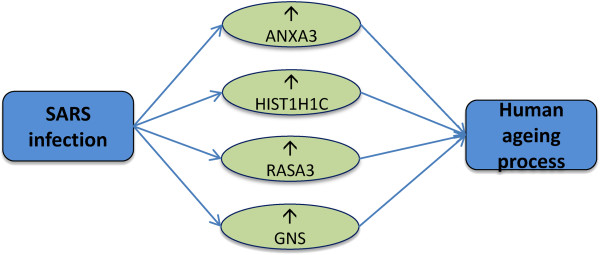
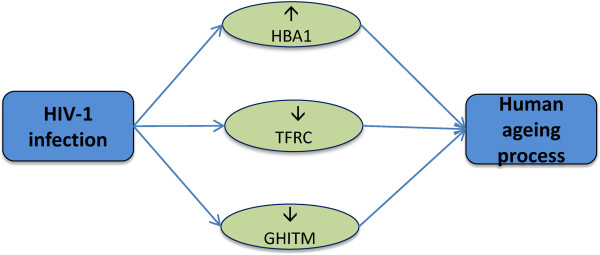
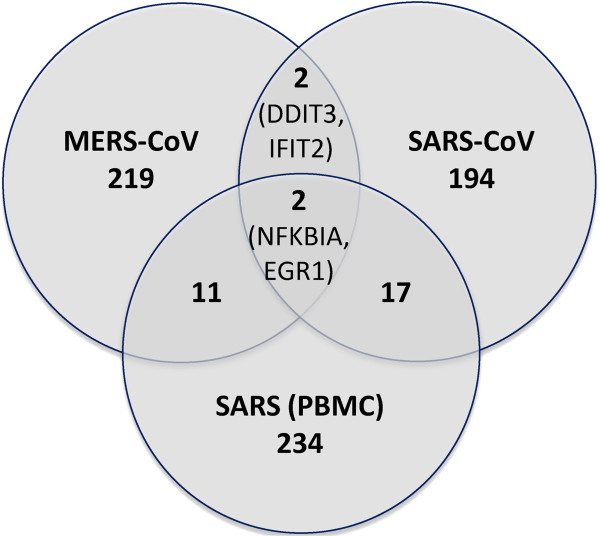
We present a quantitative framework to compare and explore comorbidity between diseases. By using neighbourhood based benchmark and topological methods, we have built comorbidity relationships network based on the OMIM and our identified significant genes. Then based on the gene expression, PPI and signalling pathways data, we investigate the comorbidity association of these 2 infective pathologies with other 7 diseases (heart failure, kidney disorder, breast cancer, neurodegenerative disorders, bone diseases, Type 1 and Type 2 diabetes). Phenotypic association is measured by calculating both the Relative Risk as the quantified measures of comorbidity tendency of two disease pairs and the ϕ-correlation to measure the robustness of the comorbidity associations. The differential gene expression profiling strongly suggests that the response of SARS affected patients seems to be mainly an innate inflammatory response and statistically dysregulates a large number of genes, pathways and PPIs subnetworks in different pathologies such as chronic heart failure (21 genes), breast cancer (16 genes) and bone diseases (11 genes). HIV-1 induces comorbidities relationship with many other diseases, particularly strong correlation with the neurological, cancer, metabolic and immunological diseases. Similar comorbidities risk is observed from the clinical information. Moreover, SARS and HIV infections dysregulate 4 genes (ANXA3, GNS, HIST1H1C, RASA3) and 3 genes (HBA1, TFRC, GHITM) respectively that affect the ageing process. It is notable that HIV and SARS similarly dysregulated 11 genes and 3 pathways. Only 4 significantly dysregulated genes are common between SARS-CoV and MERS-CoV, including NFKBIA that is a key regulator of immune responsiveness implicated in susceptibility to infectious and inflammatory diseases.
Our method presents a ripe opportunity to use data-driven approaches for advancing our current knowledge on disease mechanism and predicting disease comorbidities in a quantitative way.
感染通常与合并症相关,合并症会增加患病风险,进而可能导致更高的发病率和死亡率。严重急性呼吸综合征(SARS)是一种类似于中东呼吸综合征(MERS)病毒的威胁,但合并症是突显它们不同影响的关键因素。一位英国医生表示“比起糖尿病,我宁愿感染艾滋病毒”,因为糖尿病患者的预期寿命低于艾滋病毒感染者。然而,艾滋病毒对糖尿病有合并症影响。
我们提出了一个定量框架来比较和探究疾病之间的合并症情况。通过使用基于邻域的基准和拓扑方法,我们基于《人类孟德尔遗传》(OMIM)和我们确定的重要基因构建了合并症关系网络。然后,基于基因表达、蛋白质 - 蛋白质相互作用(PPI)和信号通路数据,我们研究了这两种感染性疾病与其他7种疾病(心力衰竭、肾脏疾病、乳腺癌、神经退行性疾病、骨骼疾病、1型和2型糖尿病)的合并症关联。通过计算相对风险(作为两对疾病合并症倾向的量化指标)和φ相关性(以衡量合并症关联的稳健性)来测量表型关联。差异基因表达谱强烈表明,SARS感染患者的反应似乎主要是先天性炎症反应,并且在不同病理状态下(如慢性心力衰竭(21个基因)、乳腺癌(16个基因)和骨骼疾病(