Xiang Shuai, Lau Wan Yee, Chen Xiao-ping
Hepatic Surgery Centre, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China.
Int J Colorectal Dis. 2015 Feb;30(2):159-71. doi: 10.1007/s00384-014-2063-z. Epub 2014 Nov 8.
Hilar cholangiocarcinoma is the most common malignant tumor affecting the extrahepatic bile duct. Surgical treatment offers the only possibility of cure, and it requires removal of all tumoral tissues with adequate resection margins. The aims of this review are to summarize the findings and to discuss the controversies on the extent of surgical resection aiming at cure for hilar cholangiocarcinoma.
The English medical literatures on hilar cholangiocarcinoma were studied to review on the relevance of adequate resection margins, routine caudate lobe resection, extent of liver resection, and combined vascular resection on perioperative and long-term survival outcomes of patients with resectable hilar cholangiocarcinoma.
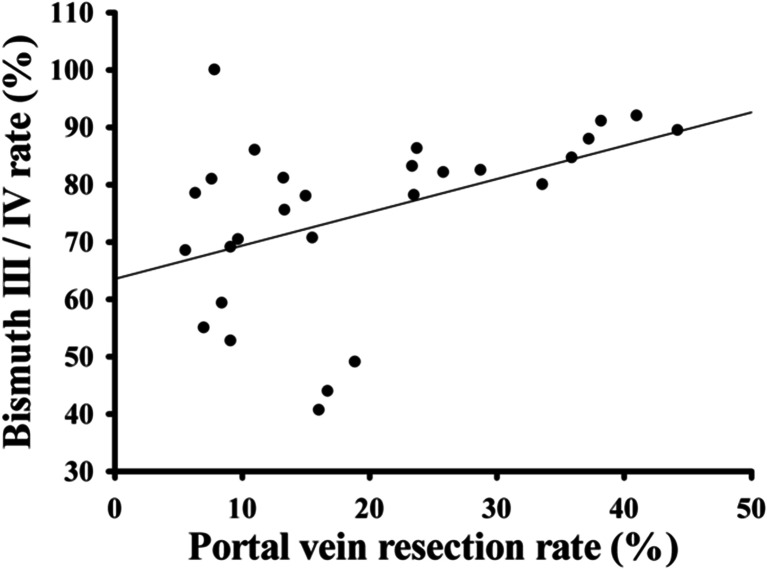
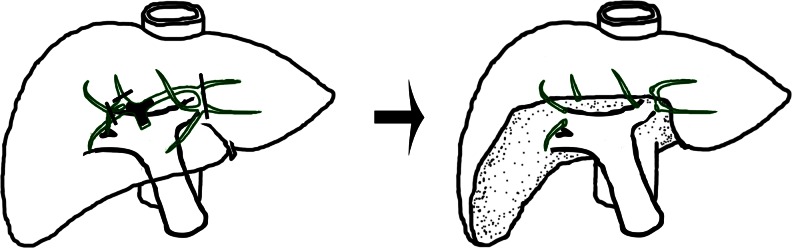
Complete resection of tumor represents the most important prognostic factor of long-term survival for hilar cholangiocarcinoma. The primary aim of surgery is to achieve R0 resection. When R1 resection is shown intraoperatively, further resection is recommended. Combined hepatic resection is now generally accepted as a standard procedure even for Bismuth type I/II tumors. Routine caudate lobe resection is also advocated for cure. The extent of hepatic resection remains controversial. Most surgeons recommend major hepatic resection. However, minor hepatic resection has also been advocated in most patients. The decision to carry out right- or left-sided hepatectomy is made according to the predominant site of the lesion. Portal vein resection should be considered when its involvement by tumor is suspected.
The curative treatment of hilar cholangiocarcinoma remains challenging. Advances in hepatobiliary techniques have improved the perioperative and long-term survival outcomes of this tumor.
肝门部胆管癌是影响肝外胆管的最常见恶性肿瘤。手术治疗是唯一可能治愈的方法,需要切除所有肿瘤组织并保证切缘足够。本综述的目的是总结研究结果,并讨论旨在治愈肝门部胆管癌的手术切除范围的争议。
研究了关于肝门部胆管癌的英文医学文献,以回顾足够切缘、常规尾状叶切除、肝切除范围以及联合血管切除对可切除性肝门部胆管癌患者围手术期和长期生存结果的相关性。
肿瘤的完全切除是肝门部胆管癌长期生存的最重要预后因素。手术的主要目标是实现R0切除。术中若显示为R1切除,建议进一步切除。联合肝切除现在即使对于Bismuth I/II型肿瘤也普遍被视为标准手术。为求治愈也主张常规进行尾状叶切除。肝切除范围仍存在争议。大多数外科医生推荐进行大范围肝切除。然而,在大多数患者中也有人主张进行小范围肝切除。根据病变的主要部位决定进行右侧或左侧肝切除。怀疑肿瘤侵犯门静脉时应考虑门静脉切除。
肝门部胆管癌的根治性治疗仍然具有挑战性。肝胆技术的进步改善了该肿瘤的围手术期和长期生存结果。