Lobo Tasso Julio, Pachon Carlos Thiene, Pachon Jose Carlos, Pachon Enrique Indalecio, Pachon Maria Zelia, Pachon Juan Carlos, Santillana Tomas Guillermo, Zerpa Juan Carlos, Albornoz Remy Nelson, Jatene Adib Domingos
Serviço de Arritmias - Eletrofisiologia e Marca-passo, Hospital do Coração de São Paulo Hcor, São Paulo, SP, Brazil.
Arq Bras Cardiol. 2015 Jan;104(1):45-52. doi: 10.5935/abc.20140167. Epub 2014 Nov 11.
Heart failure and atrial fibrillation (AF) often coexist in a deleterious cycle.
To evaluate the clinical and echocardiographic outcomes of patients with ventricular systolic dysfunction and AF treated with radiofrequency (RF) ablation.
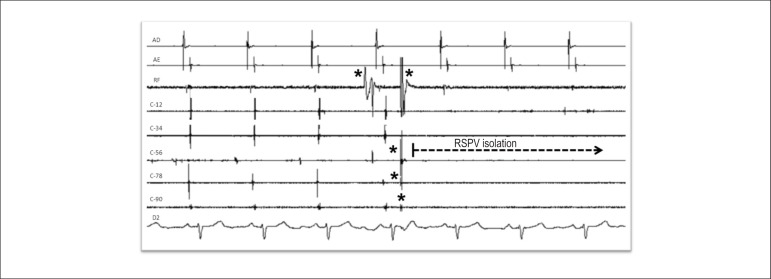
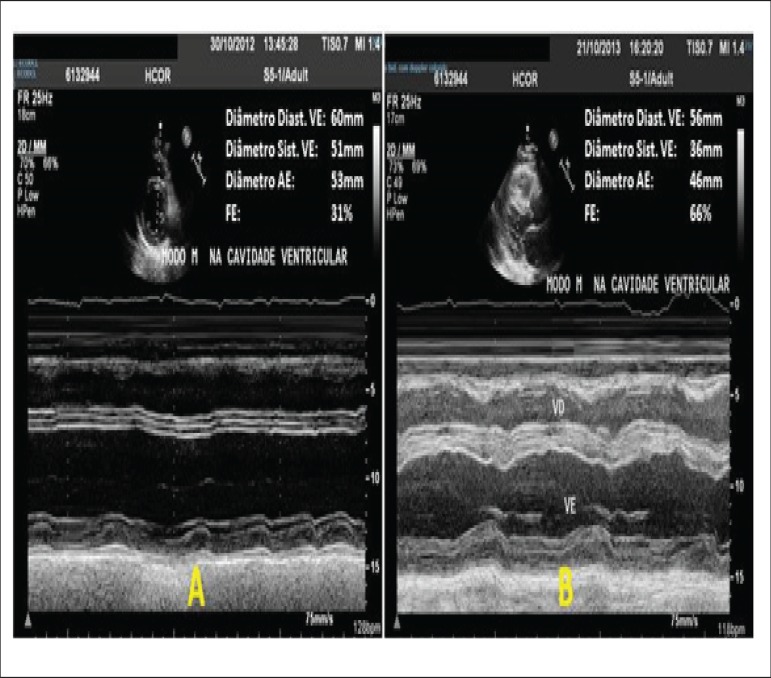
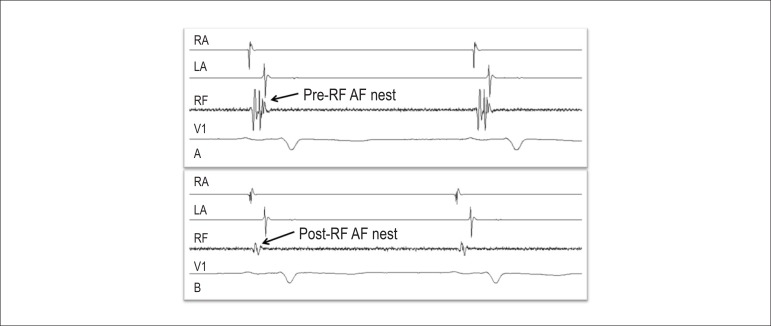
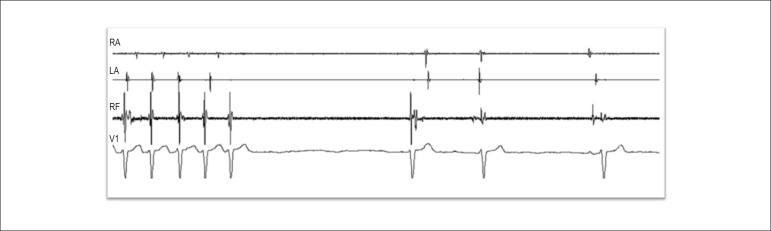
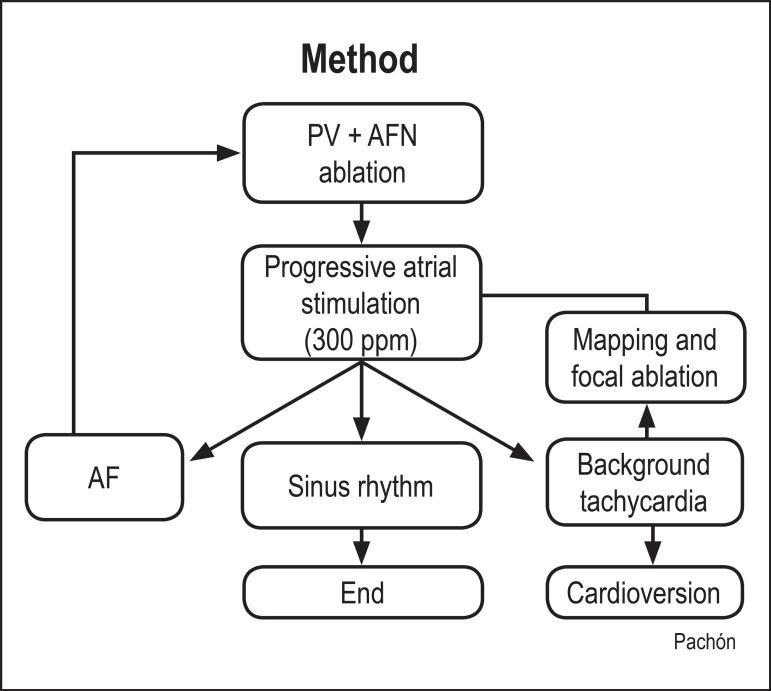
Patients with ventricular systolic dysfunction [ejection fraction (EF) <50%] and AF refractory to drug therapy underwent stepwise RF ablation in the same session with pulmonary vein isolation, ablation of AF nests and of residual atrial tachycardia, named "background tachycardia". Clinical (NYHA functional class) and echocardiographic (EF, left atrial diameter) data were compared (McNemar test and t test) before and after ablation.
31 patients (6 women, 25 men), aged 37 to 77 years (mean, 59.8 ± 10.6), underwent RF ablation. The etiology was mainly idiopathic (19 p, 61%). During a mean follow-up of 20.3 ± 17 months, 24 patients (77%) were in sinus rhythm, 11 (35%) being on amiodarone. Eight patients (26%) underwent more than one procedure (6 underwent 2 procedures, and 2 underwent 3 procedures). Significant NYHA functional class improvement was observed (pre-ablation: 2.23 ± 0.56; postablation: 1.13 ± 0.35; p < 0.0001). The echocardiographic outcome also showed significant ventricular function improvement (EF pre: 44.68% ± 6.02%, post: 59% ± 13.2%, p = 0.0005) and a significant left atrial diameter reduction (pre: 46.61 ± 7.3 mm; post: 43.59 ± 6.6 mm; p = 0.026). No major complications occurred.
Our findings suggest that AF ablation in patients with ventricular systolic dysfunction is a safe and highly effective procedure. Arrhythmia control has a great impact on ventricular function recovery and functional class improvement.
心力衰竭与心房颤动(房颤)常并存于一个有害的循环中。
评估射频(RF)消融治疗心室收缩功能障碍合并房颤患者的临床及超声心动图结局。
心室收缩功能障碍[射血分数(EF)<50%]且药物治疗无效的房颤患者在同一次手术中接受逐步RF消融,包括肺静脉隔离、房颤巢及残余房性心动过速(即“背景心动过速”)消融。比较消融前后的临床(纽约心脏协会功能分级)和超声心动图(EF、左心房直径)数据(McNemar检验和t检验)。
31例患者(6例女性,25例男性),年龄37至77岁(平均59.8±10.6岁)接受了RF消融。病因主要为特发性(19例,61%)。在平均20.3±17个月的随访中,24例患者(77%)恢复窦性心律,11例(35%)服用胺碘酮。8例患者(26%)接受了不止一次手术(6例接受2次手术,2例接受3次手术)。观察到纽约心脏协会功能分级有显著改善(消融前:2.23±0.56;消融后:1.13±0.35;p<0.0001)。超声心动图结果还显示心室功能有显著改善(EF术前:44.68%±6.02%,术后:59%±13.2%,p=0.0005),左心房直径显著减小(术前:46.61±7.3mm;术后:43.59±6.6mm;p=0.026)。未发生重大并发症。
我们的研究结果表明,心室收缩功能障碍患者的房颤消融是一种安全且高效的手术。心律失常的控制对心室功能恢复和功能分级改善有很大影响。