Roberts Martin J, Campbell John L, Abel Gary A, Davey Antoinette F, Elmore Natasha L, Maramba Inocencio, Carter Mary, Elliott Marc N, Roland Martin O, Burt Jenni A
University of Exeter Medical School, St Lukes Campus, Exeter EX1 2LU, UK.
University of Exeter Medical School, St Lukes Campus, Exeter EX1 2LU, UK
BMJ. 2014 Nov 11;349:g6034. doi: 10.1136/bmj.g6034.
To determine the extent to which practice level scores mask variation in individual performance between doctors within a practice.
Analysis of postal survey of patients' experience of face-to-face consultations with individual general practitioners in a stratified quota sample of primary care practices.
Twenty five English general practices, selected to include a range of practice scores on doctor-patient communication items in the English national GP Patient Survey.
7721 of 15,172 patients (response rate 50.9%) who consulted with 105 general practitioners in 25 practices between October 2011 and June 2013.
Score on doctor-patient communication items from post-consultation surveys of patients for each participating general practitioner. The amount of variance in each of six outcomes that was attributable to the practices, to the doctors, and to the patients and other residual sources of variation was calculated using hierarchical linear models.
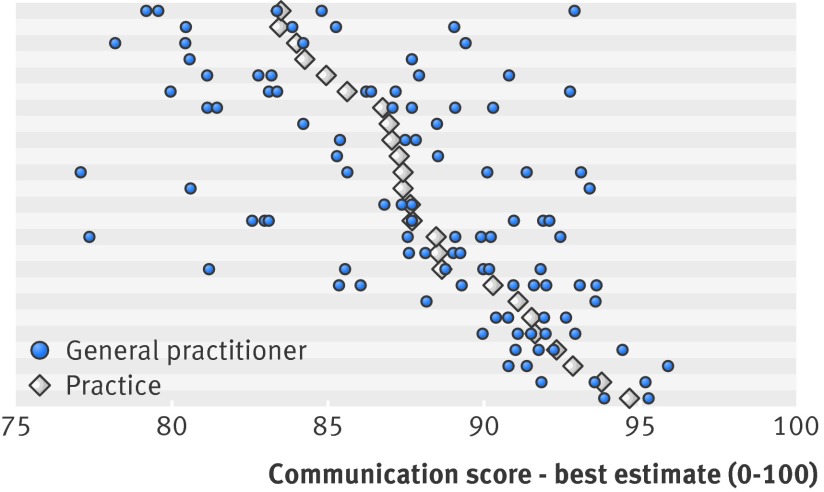
After control for differences in patients' age, sex, ethnicity, and health status, the proportion of variance in communication scores that was due to differences between doctors (6.4%) was considerably more than that due to practices (1.8%). The findings also suggest that higher performing practices usually contain only higher performing doctors. However, lower performing practices may contain doctors with a wide range of communication scores.
Aggregating patients' ratings of doctors' communication skills at practice level can mask considerable variation in the performance of individual doctors, particularly in lower performing practices. Practice level surveys may be better used to "screen" for concerns about performance that require an individual level survey. Higher scoring practices are unlikely to include lower scoring doctors. However, lower scoring practices require further investigation at the level of the individual doctor to distinguish higher and lower scoring general practitioners.
确定在一个医疗机构内,机构层面的得分在多大程度上掩盖了医生个体表现的差异。
对基层医疗服务机构分层配额样本中患者与个体全科医生面对面咨询体验的邮政调查进行分析。
选取25家英国全科医疗服务机构,这些机构在英国全国全科医生患者调查中,在医患沟通项目上具有一系列不同的得分。
2011年10月至2013年6月期间,在25家机构中与105名全科医生咨询过的15172名患者中的7721名(回复率50.9%)。
每位参与调查的全科医生的患者咨询后调查中,医患沟通项目的得分。使用分层线性模型计算六个结果中每个结果归因于机构、医生、患者及其他残余变异来源的变异量。
在控制了患者年龄、性别、种族和健康状况的差异后,沟通得分中因医生之间差异导致的变异比例(6.4%)远高于因机构差异导致的变异比例(1.8%)。研究结果还表明,表现较好的机构通常只包含表现较好的医生。然而,表现较差的机构可能包含沟通得分范围较广的医生。
在机构层面汇总患者对医生沟通技巧的评分可能会掩盖个体医生表现的显著差异,尤其是在表现较差的机构中。机构层面的调查可能更适合用于“筛查”需要个体层面调查的表现问题。得分较高的机构不太可能包含得分较低的医生。然而,得分较低的机构需要在个体医生层面进行进一步调查,以区分得分较高和较低的全科医生。