Newbould Jennifer, Abel Gary, Ball Sarah, Corbett Jennie, Elliott Marc, Exley Josephine, Martin Adam, Saunders Catherine, Wilson Edward, Winpenny Eleanor, Yang Miaoqing, Roland Martin
Cambridge Centre for Health Services Research, RAND Europe, Westbrook Centre, Cambridge CB4 1YG, UK.
University of Exeter Medical School, Smeall Building, St Luke's Campus, Exeter EX1 2LU, UK.
BMJ. 2017 Sep 27;358:j4197. doi: 10.1136/bmj.j4197.
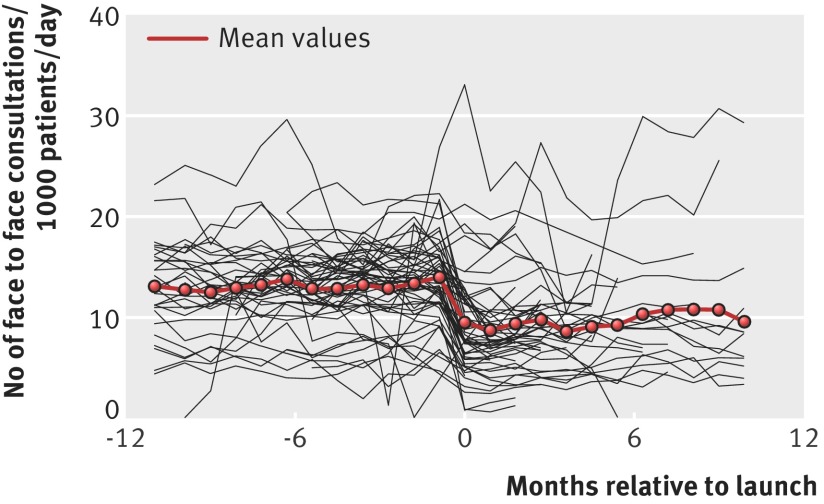
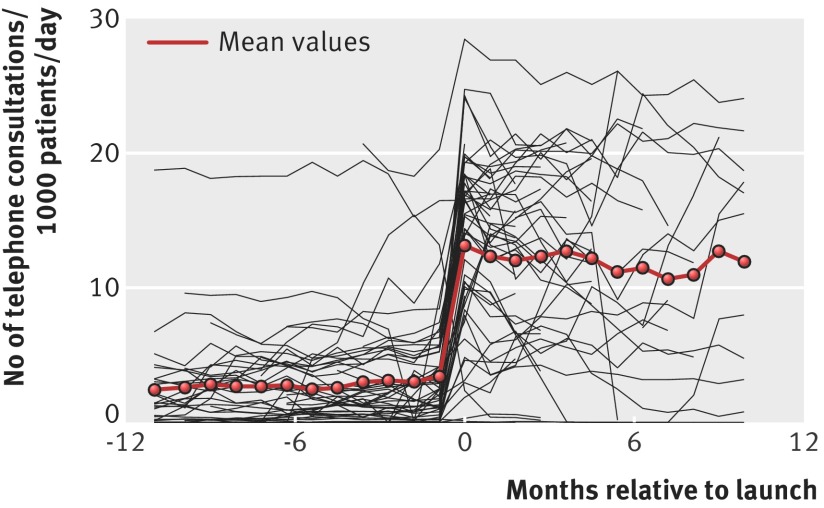
To evaluate a "telephone first" approach, in which all patients wanting to see a general practitioner (GP) are asked to speak to a GP on the phone before being given an appointment for a face to face consultation. Time series and cross sectional analysis of routine healthcare data, data from national surveys, and primary survey data. 147 general practices adopting the telephone first approach compared with a 10% random sample of other practices in England. Management support for workload planning and introduction of the telephone first approach provided by two commercial companies. Number of consultations, total time consulting (59 telephone first practices, no controls). Patient experience (GP Patient Survey, telephone first practices plus controls). Use and costs of secondary care (hospital episode statistics, telephone first practices plus controls). The main analysis was intention to treat, with sensitivity analyses restricted to practices thought to be closely following the companies' protocols. After the introduction of the telephone first approach, face to face consultations decreased considerably (adjusted change within practices -38%, 95% confidence interval -45% to -29%; P<0.001). An average practice experienced a 12-fold increase in telephone consultations (1204%, 633% to 2290%; P<0.001). The average duration of both telephone and face to face consultations decreased, but there was an overall increase of 8% in the mean time spent consulting by GPs, albeit with large uncertainty on this estimate (95% confidence interval -1% to 17%; P=0.088). These average workload figures mask wide variation between practices, with some practices experiencing a substantial reduction in workload and others a large increase. Compared with other English practices in the national GP Patient Survey, in practices using the telephone first approach there was a large (20.0 percentage points, 95% confidence interval 18.2 to 21.9; P<0.001) improvement in length of time to be seen. In contrast, other scores on the GP Patient Survey were slightly more negative. Introduction of the telephone first approach was followed by a small (2.0%) increase in hospital admissions (95% confidence interval 1% to 3%; P=0.006), no initial change in emergency department attendance, but a small (2% per year) decrease in the subsequent rate of rise of emergency department attendance (1% to 3%; P=0.005). There was a small net increase in secondary care costs. The telephone first approach shows that many problems in general practice can be dealt with over the phone. The approach does not suit all patients or practices and is not a panacea for meeting demand. There was no evidence to support claims that the approach would, on average, save costs or reduce use of secondary care.
为评估一种“先电话问诊”的方法,即要求所有希望看全科医生(GP)的患者在获得面对面咨询预约之前先与全科医生进行电话沟通。对常规医疗数据、全国调查数据和初步调查数据进行时间序列和横断面分析。将147家采用先电话问诊方法的全科诊所与英格兰其他诊所的10%随机样本进行比较。由两家商业公司提供工作量规划和引入先电话问诊方法的管理支持。咨询次数、总咨询时间(59家先电话问诊诊所,无对照)。患者体验(全科医生患者调查,先电话问诊诊所加对照)。二级医疗的使用情况和费用(医院病历统计,先电话问诊诊所加对照)。主要分析采用意向性分析,敏感性分析仅限于被认为严格遵循公司方案的诊所。引入先电话问诊方法后,面对面咨询显著减少(诊所内调整变化-38%,95%置信区间-45%至-29%;P<0.001)。平均每家诊所的电话咨询增加了12倍(1204%,633%至2290%;P<0.001)。电话咨询和面对面咨询的平均时长均有所下降,但全科医生的平均咨询总时长总体增加了8%,尽管该估计存在较大不确定性(95%置信区间-1%至17%;P=0.088)。这些平均工作量数据掩盖了诊所之间的巨大差异,一些诊所的工作量大幅减少,而另一些则大幅增加。在全国全科医生患者调查中,与其他英国诊所相比,采用先电话问诊方法的诊所患者候诊时间大幅缩短(20.0个百分点,95%置信区间18.2至21.9;P<0.001)。相比之下,全科医生患者调查中的其他得分略显负面。引入先电话问诊方法后,住院人数略有增加(2.0%,95%置信区间1%至3%;P=0.006),急诊就诊人数初期无变化,但随后急诊就诊人数的上升率略有下降(每年2%,1%至3%;P=0.005)。二级医疗费用有小幅净增加。先电话问诊方法表明,全科医疗中的许多问题可以通过电话解决。该方法并不适合所有患者或诊所,也不是满足需求的万灵药。没有证据支持该方法平均会节省成本或减少二级医疗使用的说法。