Department Psychology Health and Technology, Faculty Behavioral, Management and Social Sciences, University of Twente, Enschede, the Netherlands.
Department of Medical Microbiology, University of Groningen, University Medical Center Groningen, Groningen, the Netherlands.
Antimicrob Resist Infect Control. 2014 Oct 23;3(1):33. doi: 10.1186/2047-2994-3-33. eCollection 2014.
Antibiotic resistance is a global threat to patient safety and care. In response, hospitals start antibiotic stewardship programs to optimise antibiotic use. Expert-based guidelines recommend strategies to implement such programs, but local implementations may differ per hospital. Earlier published assessments determine maturity of antibiotic stewardship programs based on expert-based structure indicators, but they disregard that there may be valid deviations from these expert-based programs.
To analyse the progress and barriers of local implementations of antibiotic stewardship programs with stakeholders in nine Dutch hospitals and to develop a toolkit that guides implementing local antibiotic stewardship programs.
An online questionnaire based on published guidelines and recommendations, conducted with seven clinical microbiologists, seven infectious disease physicians and five clinical pharmacists at nine Dutch hospitals.
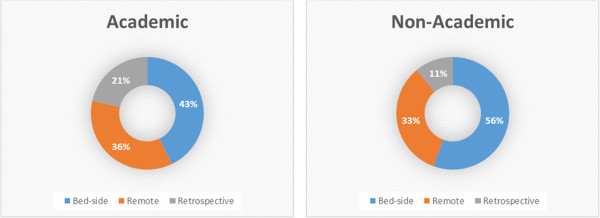
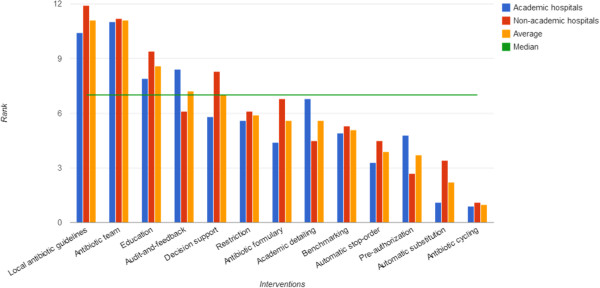
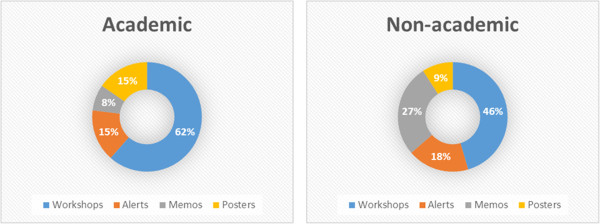
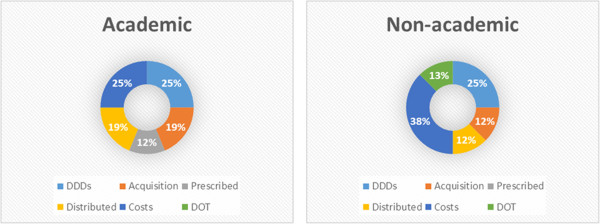
Results show local differences in antibiotic stewardship programs and the uptake of interventions in hospitals. Antibiotic guidelines and antibiotic teams are the most extensively implemented interventions. Education, decision support and audit-feedback are deemed important interventions and they are either piloted in implementations at academic hospitals or in preparation for application in non-academic hospitals. Other interventions that are recommended in guidelines - benchmarking, restriction and antibiotic formulary - appear to have a lower priority. Automatic stop-order, pre-authorization, automatic substitution, antibiotic cycling are not deemed to be worthwhile according to respondents.
There are extensive local differences in the implementation of antibiotic stewardship interventions. These differences suggest a need to further explore the rationale behind the choice of interventions in antibiotic stewardship programs. Rather than reporting this rationale, this study reports where rationale can play a key role in the implementation of antibiotic stewardship programs. A one-size-fits-all solution is unfeasible as there may be barriers or valid reasons for local experts to deviate from expert-based guidelines. Local experts can be supported with a toolkit containing advice based on possible barriers and considerations. These parameters can be used to customise an implementation of antibiotic stewardship programs to local needs (while retaining its expert-based foundation).
抗生素耐药性是对患者安全和护理的全球性威胁。为此,医院启动了抗生素管理计划,以优化抗生素的使用。基于专家的指南建议了实施这些计划的策略,但每家医院的实施方式可能有所不同。早期发表的评估基于基于专家的结构指标来确定抗生素管理计划的成熟度,但它们忽略了这些基于专家的计划可能存在有效的偏差。
分析 9 家荷兰医院利益相关者对抗生素管理计划的本地实施进展和障碍,并开发一个工具包,指导实施本地抗生素管理计划。
采用基于已发表指南和建议的在线问卷,对 9 家荷兰医院的 7 名临床微生物学家、7 名传染病医生和 5 名临床药师进行调查。
结果显示,医院的抗生素管理计划和干预措施的采用存在本地差异。抗生素指南和抗生素团队是实施最广泛的干预措施。教育、决策支持和审核反馈被认为是重要的干预措施,它们要么在学术医院的实施中进行试点,要么在为非学术医院的应用做准备。指南中推荐的其他干预措施——基准测试、限制和抗生素处方集——似乎优先级较低。根据受访者的意见,自动停止医嘱、授权前审批、自动替代、抗生素循环使用被认为不值得。
抗生素管理计划的实施存在广泛的本地差异。这些差异表明,需要进一步探讨抗生素管理计划中干预措施选择的基本原理。本研究不是报告这一基本原理,而是报告基本原理在抗生素管理计划实施中可以发挥关键作用的地方。一刀切的解决方案是不可行的,因为本地专家可能会因为障碍或合理原因而偏离基于专家的指南。可以为本地专家提供一个包含基于可能障碍和考虑因素的建议的工具包,以支持他们。这些参数可用于根据本地需求定制抗生素管理计划的实施(同时保留其基于专家的基础)。