Blohm Martin Ernst, Obrecht Denise, Hartwich Jana, Mueller Goetz Christoph, Kersten Jan Felix, Weil Jochen, Singer Dominique
Department of Pediatrics, Division of Neonatology and Pediatric Intensive Care, University Medical Center Hamburg-Eppendorf, Martinistr. 52, Hamburg, 20246, Germany.
Current address: Department of Neurology, Elbe Kliniken Stade, Bremervörder Str. 111, Stade, 21682, Germany.
Crit Care. 2014 Nov 19;18(6):603. doi: 10.1186/s13054-014-0603-0.
Electrical velocimetry (EV) is a type of impedance cardiography, and is a non-invasive and continuously applicable method of cardiac output monitoring. Transthoracic echocardiography (TTE) is non-invasive but discontinuous.
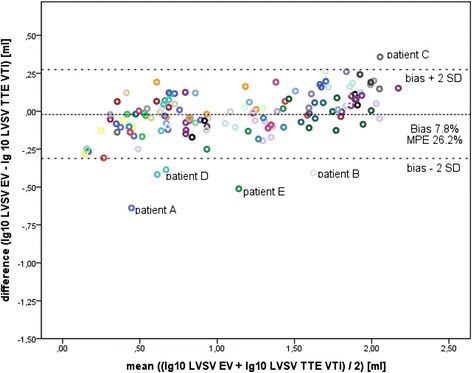
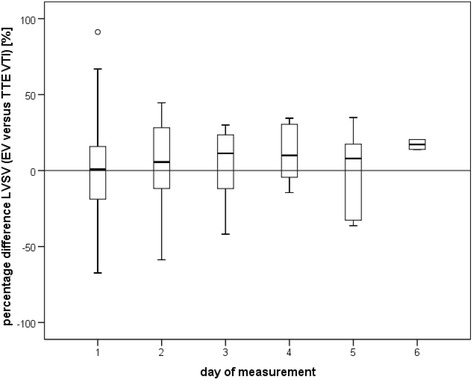
We compared EV with TTE in pediatric intensive care patients in a prospective single-center observational study. Simultaneous, coupled, left ventricular stroke volume measurements were performed by EV using an Aesculon® monitor and TTE (either via trans-aortic valve flow velocity time integral [EVVTI], or via M-mode [EVMM]). H0: bias was less than 10% and the mean percentage error (MPE) was less than 30% in Bland-Altman analysis between EV and TTE. If appropriate, data were logarithmically transformed prior to Bland-Altman analysis.
A total of 72 patients (age: 2 days to 17 years; weight: 0.8 to 86 kg) were analyzed. Patients were divided into subgroups: organ transplantation (OTX, n = 28), sepsis or organ failure (SEPSIS, n = 16), neurological patients (NEURO, n = 9), and preterm infants (PREM, n = 26); Bias/MPE for EVVTI was 7.81%/26.16%. In the EVVTI subgroup analysis for OTX, NEURO, and SEPSIS, bias and MPE were within the limits of H0, whereas the PREM subgroup had a bias/MPE of 39.00%/46.27%. Bias/MPE for EVMM was 8.07%/37.26% where the OTX and NEURO subgroups were within the range of H0, but the PREM and SEPSIS subgroups were outside the range. Mechanical ventilation, non-invasive continuous positive airway pressure ventilation, body weight, and secondary abdominal closure were factors that significantly affected comparison of the methods.
This study shows that EV is comparable with aortic flow-based TTE for pediatric patients.
电测速法(EV)是一种阻抗心动描记法,是一种无创且可连续应用的心输出量监测方法。经胸超声心动图(TTE)是无创的,但却是间断性的。
在一项前瞻性单中心观察性研究中,我们对儿科重症监护患者的电测速法与经胸超声心动图进行了比较。使用Aesculon®监护仪通过电测速法以及经胸超声心动图(通过主动脉瓣流速时间积分[EVVTI]或M型[EVMM])同时进行配对的左心室每搏输出量测量。原假设(H0):在电测速法与经胸超声心动图的布兰德-奥特曼分析中,偏差小于10%,平均百分比误差(MPE)小于30%。如有必要,在布兰德-奥特曼分析之前对数据进行对数转换。
共分析了72例患者(年龄:2天至17岁;体重:0.8至86千克)。患者被分为亚组:器官移植(OTX,n = 28)、脓毒症或器官衰竭(SEPSIS,n = 16)、神经科患者(NEURO,n = 9)和早产儿(PREM,n = 26);EVVTI的偏差/平均百分比误差为7.81%/26.16%。在OTX、NEURO和SEPSIS的EVVTI亚组分析中,偏差和平均百分比误差在原假设范围内,而PREM亚组的偏差/平均百分比误差为39.00%/46.27%。EVMM的偏差/平均百分比误差为8.07%/37.26%,其中OTX和NEURO亚组在原假设范围内,但PREM和SEPSIS亚组超出范围。机械通气、无创持续气道正压通气、体重和二期腹壁关闭是显著影响方法比较的因素。
本研究表明电测速法与基于主动脉血流的经胸超声心动图在儿科患者中具有可比性。