Wagner C L, Baggerly C, McDonnell S L, Baggerly L, Hamilton S A, Winkler J, Warner G, Rodriguez C, Shary J R, Smith P G, Hollis B W
Medical University of South Carolina Children's Hospital, Charleston, SC, USA.
GrassrootsHealth, Encinitas, CA, USA.
J Steroid Biochem Mol Biol. 2015 Apr;148:256-60. doi: 10.1016/j.jsbmb.2014.11.013. Epub 2014 Nov 13.
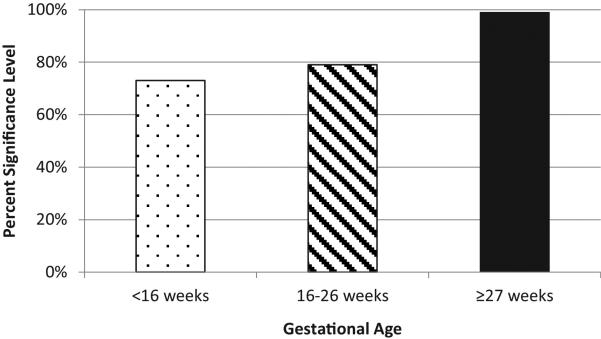
There have been observational reports that maternal vitamin D status at baseline and not closest to delivery is a better predictor of pregnancy outcomes, suggesting that a cascade of events is set into motion that is not modifiable by vitamin D supplementation during later pregnancy. To address this issue, in this exploratory post-hoc analysis using correlation and logistic regression, we sought to measure the strength of the association between serum 25(OH)D concentrations at 3 timepoints during pregnancy: baseline, 1st trimester (<16 weeks); 2nd trimester (16-26 weeks); and 3rd trimester (≥27 weeks) and preterm birth. It was hypothesized that the 25(OH)D value closest to delivery would be most significantly associated with preterm birth. To accomplish this objective, the datasets from NICHD (n=333) and Thrasher Research Fund (n=154) vitamin D supplementation pregnancy studies were combined. The results of this analysis were that 25(OH)D values closer to delivery were more strongly correlated with gestational age at delivery than earlier values: 1st trimester: r=0.11 (p=0.02); 2nd trimester: r=0.08 (p=0.09); and 3rd trimester: r=0.15 (p=0.001). When logistic regression was performed with preterm birth (<37 weeks) as the outcome and 25(OH)D quartiles as the predictor variable, adjusting for study and participant race/ethnicity, as with the correlation analysis, the measurements closer to delivery were more significantly associated and had a higher magnitude of effect. That is, at baseline, those who had serum concentrations <50nmol/L (20ng/mL) had 3.3 times of odds of a preterm birth compared to those with serum concentrations ≥100nmol/L (40ng/mL; p=0.27). At 2nd trimester, the odds were 2.0 fold (p=0.21) and at the end of pregnancy, the odds were 3.8 fold (p=0.01). The major findings from this exploratory analysis were: (1) maternal vitamin D status closest to delivery date was more significantly associated with preterm birth, suggesting that later intervention as a rescue treatment may positively impact the risk of preterm delivery, and (2) a serum concentration of 100nmol/L (40ng/mL) in the 3rd trimester was associated with a 47% reduction in preterm births. This article is part of a Special Issue entitled '17th Vitamin D Workshop'.
有观察报告表明,孕期基线时而非最接近分娩时的母体维生素D状态是妊娠结局更好的预测指标,这表明一系列事件已启动,而在妊娠后期补充维生素D无法改变这些事件。为解决这一问题,在这项使用相关性和逻辑回归的探索性事后分析中,我们试图测量孕期3个时间点(基线,即孕早期(<16周);孕中期(16 - 26周);以及孕晚期(≥27周))的血清25(OH)D浓度与早产之间关联的强度。据推测,最接近分娩时的25(OH)D值与早产的关联最为显著。为实现这一目标,将美国国立儿童健康与人类发展研究所(NICHD,n = 333)和思拉舍研究基金(Thrasher Research Fund,n = 154)维生素D补充剂妊娠研究的数据集进行了合并。该分析结果显示,与较早的值相比,更接近分娩时的25(OH)D值与分娩时的孕周相关性更强:孕早期:r = 0.11(p = 0.02);孕中期:r = 0.08(p = 0.09);孕晚期:r = 0.15(p = 0.001)。当以早产(<37周)作为结局,25(OH)D四分位数作为预测变量进行逻辑回归分析,并对研究和参与者的种族/族裔进行校正时,与相关性分析一样,更接近分娩时的测量值与早产的关联更显著且效应量更大。也就是说,在基线时,血清浓度<50nmol/L(20ng/mL)的人群早产几率是血清浓度≥100nmol/L(40ng/mL)人群的3.3倍(p = 0.27)。在孕中期,几率为2.0倍(p = 0.21),而在妊娠末期,几率为3.8倍(p = 0.01)。这项探索性分析的主要发现为:(1)最接近分娩日期时的母体维生素D状态与早产的关联更为显著,这表明后期作为挽救性治疗的干预可能会对早产风险产生积极影响;(2)孕晚期血清浓度100nmol/L(40ng/mL)与早产减少47%相关。本文是名为 “第17届维生素D研讨会” 特刊的一部分。