Cohn David E, Barnett Jason C, Wenzel Lari, Monk Bradley J, Burger Robert A, Straughn J Michael, Myers Evan R, Havrilesky Laura J
The Ohio State University, Columbus, OH, USA.
San Antonio Military Medical Center, Ft. Sam Houston, TX, USA.
Gynecol Oncol. 2015 Feb;136(2):293-9. doi: 10.1016/j.ygyno.2014.10.020. Epub 2014 Oct 23.
To estimate quality-of-life (QOL)-adjusted cost-utility with addition of bevacizumab (B) to intravenous paclitaxel/carboplatin (PC) for primary treatment of advanced-stage epithelial ovarian cancer.
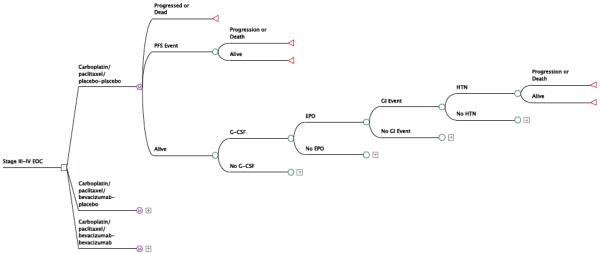
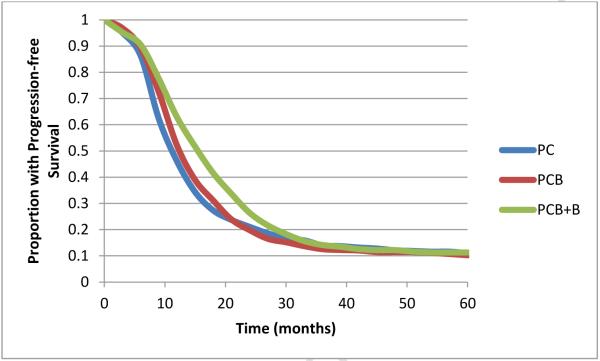
A modified Markov state transition model of 3 regimens evaluated in GOG 218 (PC, PC+concurrent B [PCB], and PCB+maintenance B [PCB+B]) was populated by prospectively collected survival, adverse event, and QOL data from GOG 218. Progression-free survival (PFS) and overall survival (OS) were modeled using primary event data. Costs of grade 4 hypertension, grade 3-5 bowel events, and growth factor support were incorporated. QOL scores were converted to utilities and incorporated into the model. Monte Carlo probabilistic sensitivity analysis was performed to account for uncertainty in estimates.
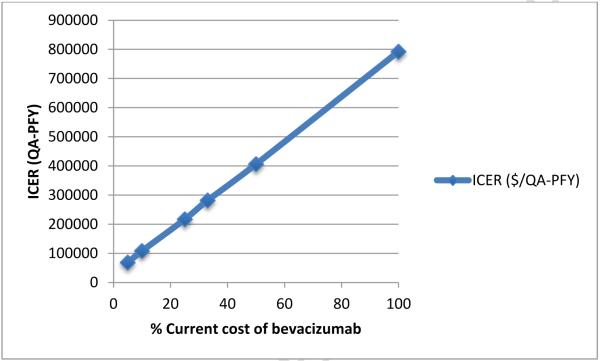
PC was the least expensive ($4044) and least effective (mean 1.1 quality-adjusted progression-free years [QA-PFY]) regimen. PCB ($43,703 and 1.13 QA-PFY) was dominated by a combination of PC and PCB+B. PCB+B ($122,700 and 1.25 QA-PFY) was the most expensive regimen with an incremental cost-effectiveness ratio of $792,380/QA-PFY compared to PC. In a model not incorporating QOL, the incremental cost-effectiveness ratio (ICER) of PCB+B was $632,571/PFY compared to PC.
In this cost-utility model, incorporation of QOL into an analysis of GOG 218 led to less favorable ICER (by >$150,000/QA-PFY) in regimens containing B compared with those that do not include B. Continued investigation of populations with ovarian cancer in whom the efficacy of treatment with bevacizumab is expected to be increased (or in whom QOL is expected to increase with use) is critical.
评估在晚期上皮性卵巢癌的一线治疗中,在静脉注射紫杉醇/卡铂(PC)基础上加用贝伐单抗(B)的生活质量(QOL)调整后的成本效用。
采用GOG 218中评估的3种治疗方案(PC、PC+同期B [PCB]、PCB+维持B [PCB+B])的改良马尔可夫状态转换模型,纳入前瞻性收集的GOG 218的生存、不良事件和QOL数据。使用主要事件数据对无进展生存期(PFS)和总生存期(OS)进行建模。纳入4级高血压、3-5级肠道事件和生长因子支持的成本。将QOL评分转换为效用值并纳入模型。进行蒙特卡洛概率敏感性分析以考虑估计中的不确定性。
PC是最便宜(4044美元)且效果最差(平均1.1个质量调整无进展年[QA-PFY])的方案。PCB(43,703美元和1.13个QA-PFY)被PC和PCB+B的联合方案所主导。PCB+B(122,700美元和1.25个QA-PFY)是最昂贵的方案,与PC相比,增量成本效益比为792,380美元/QA-PFY。在未纳入QOL的模型中,与PC相比,PCB+B的增量成本效益比(ICER)为632,571美元/PFY。
在该成本效用模型中,将QOL纳入GOG 218分析后,与不包含B的方案相比,含B方案的ICER更不理想(增加超过150,000美元/QA-PFY)。继续研究预期贝伐单抗治疗疗效增加(或预期使用后QOL增加)的卵巢癌患者群体至关重要。