Sabe Ashraf A, Dalal Rahul S, Chu Louis M, Elmadhun Nassrene Y, Ramlawi Basel, Bianchi Cesario, Sellke Frank W
Division of Cardiothoracic Surgery, Cardiovascular Research Center, Warren Alpert Medical School of Brown University, Providence, RI.
Methodist DeBakey Heart & Vascular Center, The Methodist Hospital, Houston, Tex.
J Thorac Cardiovasc Surg. 2015 Feb;149(2):613-22; discussion 622-3. doi: 10.1016/j.jtcvs.2014.10.050. Epub 2014 Oct 14.
Despite advances in surgical techniques, neurocognitive decline after cardiopulmonary bypass remains a common and serious complication. We have previously demonstrated that patients with neurocognitive decline have unique genetic responses 6 hours after cardiopulmonary bypass when compared with normal patients. We used genomic microarray to objectively investigate whether patients with neurocognitive decline had associated preoperative gene expression profiles and how these profiles changed up to 4 days after surgery.
Patients undergoing cardiac surgery underwent neurocognitive assessments preoperatively and 4 days after surgery. Skeletal muscle was collected intraoperatively. Whole blood collected before cardiopulmonary bypass, 6 hours after cardiopulmonary bypass, and on postoperative day 4 was hybridized to Affymetrix Gene Chip U133 Plus 2.0 microarrays (Affymetrix Inc, Santa Clara, Calif). Gene expression in patients with neurocognitive decline was compared with gene expression in the normal group using JMP Genomics (SAS Institute Inc, Cary, NC). Only genes that were commonly expressed in the 2 groups with a false discovery rate of 0.05 and a fold change greater than 1.5 were carried forward to pathway analysis using Ingenuity Pathway Analysis (Ingenuity Systems, Redwood City, Calif). Microarray gene expression was validated by Green real-time polymerase chain reaction and Western blotting.
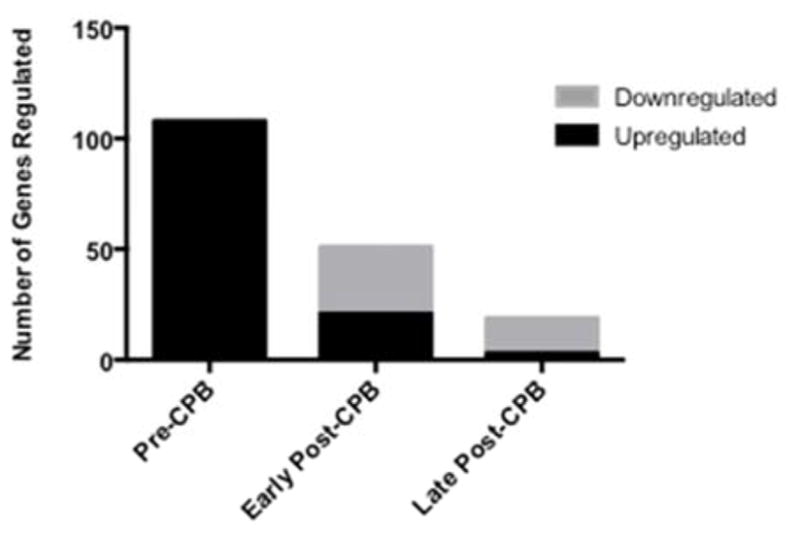
Neurocognitive decline developed in 17 of 42 patients. A total of 54,675 common transcripts were identified on microarray in each group across all time points. Preoperatively, there were 140 genes that were significantly altered between the normal and neurocognitive decline groups (P < .05). Pathway analysis demonstrated that preoperatively, patients with neurocognitive decline had increased regulation in genes associated with inflammation, cell death, and neurologic dysfunction. Of note, the number of significantly regulated genes between the 2 groups changed over each time point and decreased from 140 preoperatively to 64 six hours after cardiopulmonary bypass and to 25 four days after surgery. There was no correlation in gene expression between the blood and the skeletal muscle.
Patients in whom neurocognitive decline developed after cardiopulmonary bypass had increased differential gene expression before surgery versus patients in whom neurocognitive decline did not develop. Although significant differences in gene expression also existed postoperatively, these differences gradually decreased over time. Preoperative gene expression may be associated with neurologic injury after cardiopulmonary bypass. Further investigation into these genetic pathways may help predict patient outcome and guide patient selection.
尽管手术技术有所进步,但体外循环后神经认知功能下降仍是一种常见且严重的并发症。我们之前已经证明,与正常患者相比,神经认知功能下降的患者在体外循环后6小时有独特的基因反应。我们使用基因组微阵列客观地研究神经认知功能下降的患者术前是否具有相关的基因表达谱,以及这些谱在术后4天内如何变化。
接受心脏手术的患者在术前和术后4天进行神经认知评估。术中采集骨骼肌。将体外循环前、体外循环后6小时和术后第4天采集的全血与Affymetrix Gene Chip U133 Plus 2.0微阵列(Affymetrix公司,加利福尼亚州圣克拉拉)进行杂交。使用JMP Genomics(SAS Institute公司,北卡罗来纳州卡里)将神经认知功能下降患者的基因表达与正常组的基因表达进行比较。只有在两组中共同表达、错误发现率为0.05且倍数变化大于1.5的基因才会使用Ingenuity Pathway Analysis(Ingenuity Systems公司,加利福尼亚州红木城)进行通路分析。通过绿色实时聚合酶链反应和蛋白质印迹法验证微阵列基因表达。
42例患者中有17例出现神经认知功能下降。在所有时间点,每组的微阵列上共鉴定出54,675个常见转录本。术前,正常组和神经认知功能下降组之间有140个基因发生了显著改变(P <.05)。通路分析表明,术前,神经认知功能下降的患者与炎症、细胞死亡和神经功能障碍相关的基因调控增加。值得注意的是,两组之间显著调控的基因数量在每个时间点都有所变化,从术前的140个减少到体外循环后6小时的64个,再到术后4天的25个。血液和骨骼肌之间的基因表达没有相关性。
与未发生神经认知功能下降的患者相比,体外循环后发生神经认知功能下降的患者术前差异基因表达增加。虽然术后基因表达也存在显著差异,但这些差异会随着时间逐渐减小。术前基因表达可能与体外循环后的神经损伤有关。对这些基因通路的进一步研究可能有助于预测患者的预后并指导患者选择。